
On January 20, the World Health Organization (WHO) declared the spread of COVID-19, the disease caused by the new coronavirus SARS-CoV-2, which emerged in Wuhan, China, last December, a global health emergency.1 In response to this fast-moving outbreak, countries around the world have been seeking to implement the most effective disease prevention measures and public health emergency policies to tackle this new disease. It is interesting to note that South Korea and Japan, two close neighbors who were the first countries outside of China to have to defend against COVID-19, have implemented quite different disease prevention policies in response to the outbreak. Despite both countries having strong economic ties with China in terms of trade and tourism and being only a short airplane ride away from Wuhan, the epicenter of the outbreak, South Korea and Japan have adopted different strategies to contain the outbreak.
For example, Japan and South Korea have taken very different approaches to restrictions on travelers from China. Since February 1, Japan has denied entry to foreign nationals who had visited China’s Hubei province, which includes a home of Wuhan city, and later, on February 13, expanded that travel ban to eastern provinces including Zhejiang province. In contrast, South Korea does not prevent the entry of any foreigners who had visited China. Both countries have also adopted different approaches to their search for infected individuals. South Korea launched an aggressive testing campaign to identify as many people as possible who have been infected with the virus. As of February 27, South Korean public health authorities had tested a total of 66,652 people for the SARS-CoV-2 virus. Japan, meanwhile, reported conducting only 1,890 tests.
It seems evident that South Korea gives more weight to actively searching for and diagnosing coronavirus cases in order to break the chain reaction of disease transmission. At the same time, Japan has focused on building the public health equivalent of a firewall around the country to prevent the influx of coronavirus from overseas. Close scrutiny reveals that both pandemic prevention strategies—South Korea’s active search and Japan’s firewall approach – have advantages and disadvantages. Eventually, their respective disease prevention strategies failed, and both countries switched to encouraging social distancing (telework, school closure, etc.). This article assesses the pros and cons of both approaches, reviews the social distancing policies adopted by both countries, and argues that the United States can learn valuable lessons from the first countries outside of China who confronted the novel coronavirus.
Pros and Cons of the Active Search Strategy
Since the COVID-19 outbreak in Wuhan, the South Korean government worked hard to strengthen pandemic surveillance and quick response capabilities.2 Developing in-vitro diagnosis (IVD) capability based on reverse transcription polymerase chain reaction (RT-PCR) technology was the highest priority of the South Korean public health authorities. On February 4, the Korea Center for Disease Prevention and Control (KCDC) issued an Emergency Use Authorization (EUA) allowing the use of investigational COVID-19 IVD kits. EUA is an innovative biodefense policy adopted in response to public health emergencies. EUA allows the use of novel unapproved medical countermeasures or off-label use of approved medical countermeasures in the case of public health emergencies when no countermeasures are available. It is worth noting that South Korea officially issued the first COVID-19 related EUA in the world.3
The identification and isolation of infected individuals in order to break the disease transmission chain as quickly as possible is the heart of South Korea’s active search strategy. So far, Korea’s disease prevention efforts have worked effectively. When 28 cases were confirmed, South Korea had tested a total of 7,519 people for the COVID-19 as of February 15, 2020.4 Based on the outstanding mass-diagnosis performance of the RT-PCR kits, South Korea public health authorities could implement public health emergency policies that had successfully contained the community spread of COVID-19. The state and local governments of South Korea transparently share epidemic information about confirmed cases, follow up with all possible contacts with the confirmed cases, and test all such contacts. This approach had performed effectively during the first phase of the COVID-19 outbreak in Korea – from January 9, 2020, when the first case was confirmed, to February 17, 2020, before the 31st case came out.
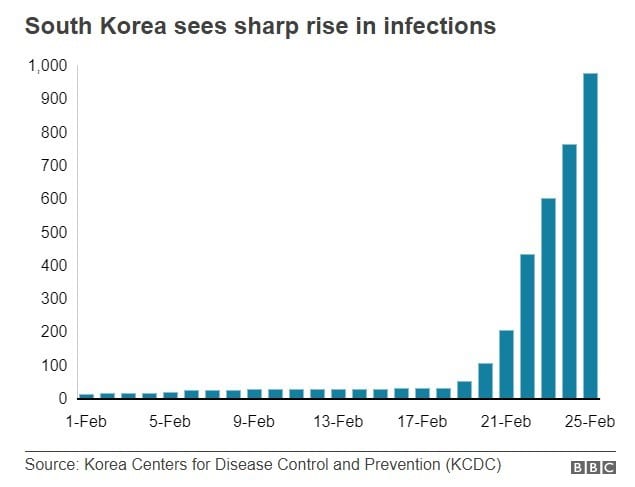
Since the 31st case was confirmed, however, South Korea entered the second phase of the COVID-19 outbreak, which reveals that there is a drawback to the existing disease prevention strategy. As seen in Figure 1, the number of COVID-19 infections began to skyrocket after February 18, when the 31st case was confirmed. The 31st case was associated with a religious group called the Shincheonji Church of Jesus.6 That case was responsible for infecting 14 of the 20 new cases that KCDC reported on February 19.7 The governor of Gyeonggi Province issued a search and seizure warrant, and investigators discovered that the church had provided KCDC with incorrect information about its members and the list of participants in the church service attended by the 31st case. An epidemiological investigation by public health authorities also revealed the church had lied and hid their travel history to Wuhan. As of March 1, of the 3,526 confirmed cases and 93,456 suspected cases, 59.9% of the confirmed cases were originated from the church services.8
This case illustrates that active participation and supports from all citizens are required to achieve successful disease prevention using the active search strategy. If one person or a group does not follow the government’s guidelines, this can create a critical loophole that can disrupt all disease prevention efforts. As a result of this breakdown in the public health response based on active search , the government has faced increasing criticism for its decision not to ban all people visiting and staying in China from entering South Korea.9
Pros and Cons of the Firebreak/Firewall Strategy
Unlike South Korea’s disease prevention efforts to identify and isolate infected individuals already in the country, Japan put more effort into building a firewall against the influx of COVID-19 cases from overseas. The main features of this strategy are bans on the entry of travelers from hard-hit regions of China and quarantines for travelers arriving from other countries/regions with active COVID-19 outbreaks. The Japanese public health strategy is similar to the Japanese military concept of “mizugiwa sakusen (水際作戦),” which refers to the military doctrine of repelling invaders as soon as they reach the shore,. Based on the concept of “mizugiwa,” Japan has developed a disease prevention approach whose goal is to prevent the importation of infectious disease into Japan. Prime Minister Shinzo Abe emphasized the importance of blockade at a meeting regarding the COVID-19 crisis, in addressing “we need to take action to implement a more comprehensive and agile border control to stop the inflow of the infectious disease into Japan.”10 Indeed, Japan proactively imposed travel restrictions and raised a bar of entry to blockade around the country. On February 1, the Japanese government banned entry by foreign nationals who had visited Hubei province and ten days later extended the entry ban to people holding Chinese passports issued in the eastern provinces of China, such as Zhejiang province, which were also suffering from COVID-19. Also, on February 26, Japan banned entry by foreign nationals who have visited Daegu – the epicenter of the South Korea’s second phase outbreak – and neighboring county of Cheongdo.
Harbors and airports are core strategic points of the Japanese “mizugiwa” defensive line. The best example of the Japanese mizugiwa concept of disease prevention is the case of the Diamond Princess cruise ship. On February 4, the Japanese government prevented the people onboard the Diamond Princess from disembarking but forced them to stay on the ship anchored in Yokohama harbor. The quarantined ship became a breeding ground for coronavirus, and more than 700 cases are reported from the people on-board in a terrible state of neglect. The crew and passengers were finally disembarked on March 1, but the number of deaths from the on-board people are still increasing. On March 7, one infected passenger in the ship died, bringing the death toll from the ship to seven. According to Dr. Amesh Adalja of the Johns Hopkins Center for Health Security, “The quarantine was not justified, and violated the individual rights of the passengers while allowing the virus to literally pick them off one-by-one.”11 This quarantine was identical to the medieval age tactic of not allowing ships to disembark passengers until they underwent a public health inspection and received a “clean bill of health.” If the ship didn’t pass the inspection, the crew and passengers had to remain anchored offshore for at least forty days to prove they have no disease. It is telling that Japan is attempting to confront a pandemic in the 21st century with a disease prevention strategy that emerged in the medieval ages.
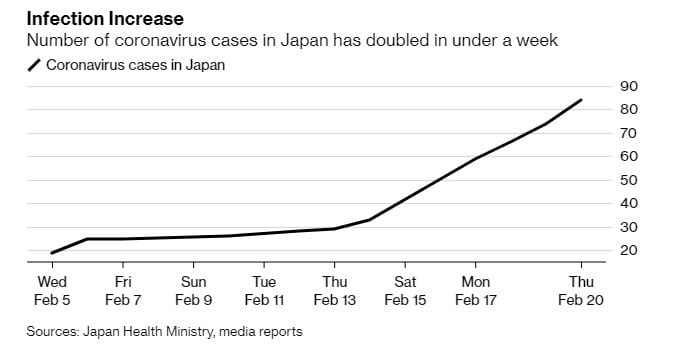
As seen Figure 2, by early February, the Japanese defensive line for disease prevention had worked well at preventing the entry of SARS-CoV-2 into Japan. However, the number of COVID-19 confirmed cases were increasing in Japan regardless of the Japan’s strenuous effort to blockade the inflow of COVID-19 from overseas such as the Diamond Princess case. On February 16, Japan’s health minister acknowledged that the government fails to track the route of infections in the country, which exposes a Japan’s weakness to respond to a public health emergency.13
Japanese people criticize that the government has not seriously considered implementing an active search strategy to detect suspected cases, which contributes to cutting a chain reaction of disease transmission. Although the Japanese government announced that it has the capacity to test 3,800 samples a day, only 8,111 cases had been tested by March 4. There was a case that a public health center denies diagnostic testing for a patient who needs it because of strict restrictions.14 Under the Japanese government guidelines, people who have cold-like symptoms, a fever of 37.5 Celsius or extreme tiredness or breathing problems for four days or more are eligible for hotline consultation on whether they should get tested. Due to the inadequate testing scheme, experts estimate that current Japan’s coronavirus situation is likely already much higher than reported, with the reported infection rate suspected to be just the “tip of the iceberg.15 Lack of information about the sources and routes of infection, and the overall risk of community spread, will likely fuel public anxiety in Japan as the number of confirmed cases continues to rise.
The Japanese case reveals that the defensive line approach to blockade the inflow of infectious diseases is not the most effective disease prevention policy. It proves that there is no perfect firewall to blockade incoming diseases in the contemporary world where the interdependence of states is high. Fearful of the impact on the tourist industry, Japan chose not to implement a comprehensive entry denial to all Chinese, but only a partial denial of foreign nationals who had visited hard-hit regions of COVID-19. Building a firewall with a hole in the middle guarantees that a “mizugiwa”-style strategy will not work.
Lessons learned from both South Korea and Japan cases
The South Korea and Japan cases give us a question – which disease prevention strategy is more effective to deal with pandemics between the active search and the defensive line. It is complicated to provide a clear answer because there are many intervening variables for comparing these countries. Nevertheless, these case studies clearly show that both strategies have pros and cons. Countries facing COVID-19 outbreak such as the United States should mix and match from these two strategies to protect their citizens. South Korea’s active search efforts have contributed to containing the chain reaction of disease transmissions in the community, but public cooperation is essential. A single person or group who fails to comply with the government’s guidance may disrupt the entire disease prevention campaign. On the other hand, Japan tried to establish a firewall around the country to protect its people from an incoming disease, but in this globalized era there were too many holes in the firewall to prevent the virus from entering Japan. These case studies illustrate that it is necessary to combinate the two different strategies simultaneously – establishing a strict defense line outside along with active searching inside.
Although the United States has adopted its own version of the mizugiwa strategy16, the experience of Japan demonstrates that it is not possible for a country to hermetically seal its borders. The United States, with its more numerous ports of entry and longer land borders, would be even more hard-pressed than the island-nation of Japan to successfully implement mizugiwa. The South Korean experience demonstrates the value of the active search strategy to identify and isolate infections as quickly as possible to break the chain of disease transmission. However, the South Korean experience also shows that the overall volume of diagnostic testing is not the sole, or even most important indicator, of an effective public health response. Governments also need to earn the trust of their citizens so they will cooperate with the public health authorities.
Japan and South Korea were unfortunate enough to be among the first countries in the world to confront the novel coronavirus after China. The coronavirus outbreak in both Japan and South Korea overwhelmed their early efforts at prevention and both countries are now adopting social distancing policies to contain the spread of the disease. The United States should take advantage of the lessons learned from both of these countries in devising the next phase of its response to the coronavirus pandemic.
REFERENCES
1. World Health Organization (WHO), WHO Director-General’s statement on IHR Emergency Committee on Novel Coronavirus (2019-nCoV, posted on 30 January 2020, available at https://www.who.int/dg/speeches/detail/who-director-general-s-statement-on-ihr-emergency-committee-on-novel-coronavirus-(2019-ncov)
2. Lee Han-soo, ‘Biosurveillance essential as no leader want absence of information during health crisis,’ Korea Biomedical Review, published December 16, 2019, available at http://www.koreabiomed.com/news/articleView.html?idxno=6998
3. South Korea and the United States issued EUA on the same day (Feb 4, 2020), but Korea (GMT+9) announced earlier than the United States (GMT-5), given the different time zone.
4. Korea Center for Disease Prevention and Control (KCDC), The Updates of COVID-19 in Republic of Korea as of 15 February, 2020, press released on 15 February, 2020, available at KCDC website in English https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030
5. The figure is sourced from BBC news, “Coronavirus: Why did infections shoot up in South Korea?” posted on Feb 25, 2020, available at https://www.bbc.com/news/world-asia-51609840
6. The 80th General Council of the Presbyterian Church of Korea in 1995 and other major Christianity groups stipulate Shincheonji Church of Jesus as an anti-social and heretic group, see The Korea Economic Daily, posted on Feb 19, 2020, available at https://www.hankyung.com/life/article/2020021986767
7. Sangmi Cha, Jack Kim, South Korea reports 20 new coronavirus cases, church services at center of outbreak, Reuters, posted on Feb 18, 2020, available at https://www.reuters.com/article/us-china-health-southkorea-cases/south-korea-reports-20-new-coronavirus-cases-church-services-at-center-of-outbreak-idUSKBN20D02O
8. Korea Center for Disease Prevention and Control (KCDC), The Updates of COVID-19 in Republic of Korea as of 1 March, 2020, press released on March 1, 2020, available at KCDC website in English
9. Steven Borowiec, How South Korea’s Coronavirus Outbreak Got so Quickly out of Control, TIME, posted on Feb 24, 2020, available at https://time.com/5789596/south-korea-coronavirus-outbreak/
10. The Asahi Shimbun, “Japan bans entry from 2nd Chinese province, raises travel advisory,” posted on Feb 12, 2020 available at http://www.asahi.com/ajw/articles/13121171
11. Morgan McFall-Johnsen, How the ‘failed’ quarantine of the Diamond Princess cruise ship started with 10 coronavirus cases and ended with more than 700, Business Insider, posted on Feb 28, 2020, available at https://www.businessinsider.com/how-diamond-princess-cruise-ship-coronavirus-quarantine-went-wrong-2020-2
12. Gearoid Reidy, As Cases Mount, Japan Rapidly Becomes a Coronavirus Hotbed, Bloomberg, posted on Feb 19, 2020, available at https://www.bloomberg.com/news/articles/2020-02-19/as-cases-mount-japan-is-rapidly-becoming-a-coronavirus-hotbed
13. Adam Minter, Japan Can’t Run Out the Clock on Coronavirus, Bloomberg Opinion, posted on Feb 21, 2020, available at https://www.bloomberg.com/opinion/articles/2020-02-21/japan-can-t-run-out-the-clock-on-covid-19
14. The Mainichi, Japan Medical Assoc. to probe public health centers’ refusal to conduct coronavirus tests, posted on Feb 27, 2020 available at https://mainichi.jp/english/articles/20200227/p2a/00m/0na/006000c?mode=print
15. Masahiro Kami, the executive director of Japan’s Medical Governance Research Institute, Interviewed with CNN; see Will Ripley et al., Japan’s coronavirus infection rate could be ‘tip of the iceberg’ as experts call for more testing, CNN, posted on Mar 5, 2020
16. Donald J. Trump, President of the United States, tweeted on March 10, 2020, available at https://twitter.com/realDonaldTrump/status/1237334397172490240
ABOUT THE AUTHOR
HyunJung Kim (Henry Kim) is a current PhD student in Biodefense at George Mason University, whose works primarily focuses on the use of unapproved medical countermeasures in response to public health emergencies as well as the historical study of biological warfare. He holds a Master’s in National Security Studies from California State University, San Bernardino, and Bachelor’s Degrees in Sociology and Public Administration from Korea University. He additionally served in as an intelligence officer in the Republic of Korea (ROK) Army. Contact him by email: hkim76@gmu.edu
REPUBLISH THIS ARTICLE
You may republish this article under the terms of the Creative Commons Attribution-NoDerivatives 4.0 International License (CC BY-ND 4.0)
– Clearly credit the author
– Do not materially change the content of the article
– Include a link-back before or after article, e.g. This article is courtesy of Global Biodefense. Read the original article here (insert hyperlink)
Not all articles on Global Biodefense are available for CC BY-ND 4.0 licensing. Any available for republishing are clearly marked. Please contact us with any questions on usage terms or how to contribute articles as a guest author.