The use of bioweapons is not a new concept, having been employed since at least ancient Greece as a mechanism for attacking enemy populations. In the present day, cases like the Amerithrax attacks of 2001 and the Rajneeshees cult’s use of salmonella in Oregon restaurants point to successful use of bioweapons. However the actual cases of use by terrorist groups are few and far between. Terrorism of any form has both pros and cons, but given the historical use of bioterrorism and its success, why has it not steadily increased in application like suicide bombings?
Contributing author Saskia Popescu, MPH examines the barriers that non-state actors face when contemplating, designing, and deploying biological weapons in the United States and the impact such barriers have on the attractiveness of bioweapons for terrorist groups.
Introduction: A Background on Bioweapons
PURPOSE
Biological weapons have been probably utilized at least since the time of the ancient Greeks as a means to kill or weaken enemy populations. Scholars credit the first written conceptual account of bioweapon use to stories about Hercules. The mythological Greek hero, after slaying the Hydra, dipped his arrows in its toxic blood. From this, some historians say, the first depiction of bioterrorism was introduced into the Western world (Mayor, 2003). In many ways, this mythological depiction became a reality when plague-infected corpses were thrown over the city walls of Kaffa and English settlers gave smallpox riddled blankets to Native Americans (Alchon, 2003, Oldstone, 2010). In modern times, non-state actors have used bioterrorism as a means of swaying political votes, instilling fear in people, and reinforcing apocalyptic ideology.
Internationally and domestically, bioterrorism is considered by some as a very real threat, with the United States being considered especially vulnerable. Experts are divided in this notion, with some positing the realistic threat of terrorists using bioweapons, while others say this threat is wholly blown out of proportion. Tucker states that “much of the discussion to date has focused on the vulnerability of large cities to terrorist attacks, while neglecting a careful assessment of the threat” (Tucker, 2000). The threat of bioterrorism and capabilities of those considering its utilization are components that must truly be addressed to better respond to and prevent such events.
Understanding the Threat of Biological Weapons and U.S. Vulnerability
The heightened sense of vulnerability after the 2001 anthrax attacks in the United States attacks has brought bioterrorism to the forefront of public attention (Koblentz, 2009). In 2008, the Department of Homeland Security (DHS) stated that, “the threat posed by biological agents employed in a terrorist attack on the United States is arguably the most important homeland security challenge of our era. Even if there are fewer casualties, additional second-order consequences (including psychological, social, and economic effects) would dramatically compound the effects” (Radosavljevic, 2009).
The anthrax attacks of 2001, coined the Amerithrax attacks, revealed a deep-seeded vulnerability within the U.S. During those attacks, 20 billion anthrax spores were released from half a teaspoon of powder. Infecting 22 known people and resulting in 5 deaths, this case of bioterrorism cost roughly $6 billion (Thompson, 2006). While it was later reported that an American scientist, Dr. Bruce Ivins, was the main suspect for the Amerithrax attacks, there continues to be fake attacks involving baby powder and other faux anthrax. Moreover, there are indeed terrorist organizations that have sought to use bioweapons. Al Qaeda leader Abu Hamza al-Muhajir stated in a 2006 audiotape that he implored scientists and experts to join al Qaeda in the testing and creation of biological weapons (Thompson, 2006). The attention that bioterrorism garners has far reaching consequences that cause economic, psychological, and political disruptions.
Yet the reality of these weapons suggests a more lackluster outcome. Attacks like those of the Rajneeshees cult in Oregon, which infected hundreds of people with salmonella, are considered success stories, but cults like Aum Shinrikyo, which had the monetary means to employ these weapons, never experienced that kind of success. Indeed, because it is impossible to completely defend against all attacks, threat assessment is crucial. The disputed degree of U.S. vulnerability has become even more heated among scientists, with some arguing that the U.S. may have over-assessed the threat (Thompons, 2006).
Many subject matter experts have pointed to the instantaneous wave of federal support that biodefense received after the Amerithrax attacks, and that while this support was needed, there was little assessment into the realities of the bioterrorist threat. Relatively little effort has been made to determine the threat of terrorist use of bioterrorism; instead, the U.S. has focused on internal vulnerabilities. Dr. Leitenberg points out that “within 4 years, almost $30 billion in federal expenditure was appropriated to counter the anticipated threat. This response took place in the absence of virtually any threat analysis” (Leitenberg, 2005). Vulnerability is an ongoing reality, but one must also consider whether the threat of bioweapons is as great as the U.S. government previously estimated.
Thesis Argument
While there is an undeniable U.S. vulnerability to bioweapons attack, the lack of capabilities to carry out such attacks has perhaps created a hypersensitivity to such threats. Non-state actors have in the past, and will continue in the future, to consider and employ the use of bioweapons. However, through an analysis of past, small-scale attacks in the U.S., the barriers to successful large-scale bioterrorism can be identified. Diffusion-of-innovation studies address why and at what rate new ideas (such as technologies) spread throughout a culture or society.
The most popular example Rogers points to is the unsuccessful attempt to improve sanitation and health in Peru during a health two-year health campaign. The project focused on boiling water and the link between sanitation and illness but was largely deemed a failure because campaign workers failed to identify the social norms and beliefs that saw boiled water as diseased. Rogers pointed out that the societal habits and norms within a society will outweigh the innovation regardless of its benefit to them (Rogers, 1983). In effect, this theory discusses the question of why certain ideas become popular while others never take off. With this concept in mind, analyzing why bioweapons have proven their efficacy, yet have not been utilized on a large-scale by non-state actors, reveals substantial barriers to utilization
This thesis seeks to point out the substantial hurdles non-state actors face when attempting to use bioweapons. It will do this by addressing several key points in the process of using bioweapons, from procuring the agent to dissemination and even to the impact of environmental conditions. An analysis of specific historical cases of bioterrorism through such a capabilities assessment will demonstrate the prevalent deterrents terrorists face when considering and deploying bioweapons.
In the Weapons of Mass Destruction Commission’s 2006 Bioterrorism and Threat Assessment, threat assessment is broken down into a diagram as shown in Figure 1 (Ackerman, 2006). The diagram in Figure 1 and equation in Figure 2 address the role of threat, likelihood of attack, motivation, capability, vulnerability of assets, hazard posed, and value. In the past, assessments of bioterrorism have focused on only a small section of these variables, mainly the consequences of attacks, value of assets being defended, and vulnerabilities.
This analysis will focus on the capabilities and motivations of potential bioterrorists and assess their impact on actual usage of bioweapons.
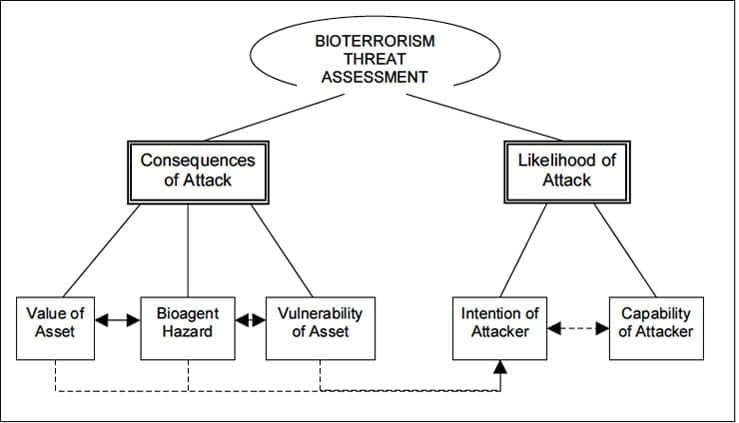
Figure 1 presents these components, indicating the relationship between the intention and capability of an attacker. The equation demonstrated in Figure 2 also relays the importance of capabilities and motivation in the equation regarding threat of attack. This equation points to the role of intent, vulnerability, and capabilities in regards to the threat of an attack (Thompson, 2006). Previous analyses have focused on the vulnerability component of this equation. The emphasis on capabilities and motivation is the driving force behind this analysis in order to provide a better understanding of terrorist capabilities when pursuing bioterrorism. This thesis will attempt to do this through an analysis of the hurdles that inhibit utilization.

BACKGROUND
Bioterrorism has several definitions, but the most prevailing understanding is, “the use by non-state actors of microorganisms (pathogens) or the products of living organisms (toxins) to inflict harm on a wider population” (Ackerman, 2006). Bioterrorism employs bioweapons (BW) as a means of inflicting harm, morbidity and mortality, economic loss, psychological distress, and general turmoil upon a group of people.
Biological Weapons
The Centers for Disease Control and Prevention (CDC) has categorized biological agents based on several variables including their “ease of dissemination or transmission from person to person”, the degree to which they “result in high mortality rates and have the potential for major public health impact” and the degree to which they might “cause public panic and social disruption, and require special action for public health preparedness” (CDC, n.d.). By using this categorization, health agencies around the world are able to help first responders and public health personnel to identify and understand biological agents that pose an increased risk for use in terrorism. The categories defined by the CDC are:
Category A agents can be easily disseminated or transmitted from person to person, result in high mortality rates and have the potential for major public health impact. They might cause public panic and social disruption, and they require special action for public health preparedness. Examples: Anthrax, botulism, plague, smallpox, tularemia, and viral hemorrhagic fevers (VHF).
Category B agents are moderately easy to disseminate, result in moderate morbidity rates and low mortality rates, and require specific enhancements of CDC’s diagnostic capacity and enhanced disease surveillance. Examples: Q fever, glanders, typhus, and ricin toxin.
Category C agents include emerging pathogens that could be engineered or disseminated in the future due to their availability, ease of production and dissemination, and potential for high morbidity and mortality rates and major health impacts. Examples: emerging infectious diseases like Nipah virus and hantavirus.
Food or Waterborne Agents/Food Safety Threat – Salmonella species, Shigella dysenteria – Shigella, Escherichia coli 0157:H7 –E. coli, Vibrio cholerae – Cholera, Cryptosporidium – Crypto, Norviruses – Noro, Clostridium botulinum neurotoxin – botulism, and typhus (typhoid fever).
Effects of Bioweapons
Biological weapons are unique in their capacity not only to cause delayed morbidity and mortality as a result of their incubation periods, but also to spread disease. Unlike a bomb, bioweapons can cause delayed illness and transmission of infection among people. A delay in illness due to an extended incubation period might allow an infected person to travel and potentially expose hundreds or thousands of people, as some illnesses allow a host to be infectious before they are symptomatic. On the other hand, the ability to spread disease from person to person is a wholly unique component of bioweapons. Consider the Category A agents: several of them are highly contagious, such as pneumonic plague and smallpox. Bioweapons like plague are both endemic (naturally occurring) and transmissible through droplets, creating an exposure within six feet of the infected individual. These pathogens are incapacitating but also take several days to cause illness.
Should the motive be to inflict injury and create a drain upon the medical system, all of these agents are especially effective in causing physical harm, but two in particular cause substantial damage. Organisms like anthrax and botulism that cause respiratory failure pose a particularly large burden, as they often require mechanical ventilation and specialist medical care. These pathogens are capable of causing an incapacitating illness and preventing individuals from performing their daily duties, but only a few are communicable between people. Organisms like anthrax, tularemia, and botulism are not known to spread between individuals beyond bloodborne pathogen exposure. Plague, VHF, and smallpox however, are extremely communicable, making their ability to cause downstream effects substantially more significant.
The Category A agents are all unique in their manifestation, but several of them initially manifest like influenza, which can delay treatment and increase the risk of exposure and death. Several studies have revealed the inability of physicians to correctly diagnosis cases of Category A agents, compounding their effects that much more (Cosgrove, 2005). Overall, the pathogens considered as possible bioweapons all pose devastating health consequences to the infected person, and some of them create unique challenges for clinicians regarding both diagnosis and treatment. The ability to transmit disease and have delayed presentation makes these weapons especially sinister and potentially all the more appealing to terrorists.
Historical Use of Bioweapons
Bioterrorism is by no means a novel concept. While Hercules is noted to be the first Western literary example, the reality dates back just as far. The Greek historian Herodotus in the 5th century BCE described Scythian archers using poison-tipped arrows against their enemies. The Scythians would also create a mixture of decomposed venomous snakes and dung, sealed and made especially potent over time, that they would cover their arrows in. This potent concoction would infect victims with a dangerous mixture of bacteria like tetanus and gangrene (Johnson, n.d.). The most commonly acknowledged case of bioweapons use is from the late 14th Century CE, in the city of Kaffa. During their besieging of the city, the Tartar army catapulted the bodies of plague victims over the city walls. Inhabitants and travelling merchants became infected with plague, bringing the deadly disease back to Italy and sparking the spread of the Black Death, killing an estimated 30-60% of the European population (Alchon, 2003).
More recently, in 1763 European settlers gave smallpox-laden linens to Native Americans in America, wiping out entire communities due to of a lack of immunity (Oldstone, 2010). Covert missions during World War I by the Germans infected Romanian sheep with anthrax, intending to infect their Russian purchasers (Carus, 2002). After several other experiments and cases during World Wars I and II, the Biological Weapons Convention (BWC), also called Biological and Toxin Weapons Convention (BTWC), was negotiated. As the first multilateral disarmament treaty, it banned the “development, production, and stockpiling of an entire category of mass destruction” (UN, n.d.). Signed in 1972, it entered into force in 1975 and worked to end state-sponsored bioweapons programs. The Second Review Conference in 1986 “agreed that the States Parties were to implement a number of confidence building measures (CBM) in order to prevent or reduce the occurrence of ambiguities, doubts and suspicions and in order to improve international co-operation in the field of peaceful biological activities” (UN, n.d.). Signatory states were to provide annual reports related to BWC data, research centers and vaccine production.
While the BWC has helped prevent states’ use of bioweapons, a few individuals and groups have continued seeking bioweapons to use for their purposes. Seth Carus, in a 2002 study, extensively addressed the cases of biocrimes worldwide since 1990, citing the use of bioweapons by terrorists, criminals (those motivated by personal revenge or financial gain objectives), and other/uncertain (cases where the perpetrator was unknown). Carus provides the most extensive review of biocrime cases from 1990-2002. If bioterrorism has occurred since Carus’s analysis, there has been little to no unclassified information to document it. The few recent ricin cases that have been received media attention involved individuals sending castor beans (non-weaponized ricin) to federal officials and gun control organizations. Several experts have pointed to the over-hyped attention these cases have received, especially since these attempts yielded no illness and were using non-toxic substances (Garza, 2013).
Carus in his study noted that, “to date, few terrorists have demonstrated an interest in bioterrorism, and fewer still tried to acquire biological agents. Unclassified accounts mention at least 54 cases in which a terrorist group allegedly had an interest in bioweapons, but there is little evidence to confirm most of these cases” (Carus, 2002). Of these 54 cases, only 27 have more than minimal evidence that a terrorist group actually acquired, attempted to acquire, or threatened to use a bioweapon. Eight of these cases produced evidence that the terrorist group actually acquired the agent, but in only five cases did terrorists confirm the use or attempted use of biological weapons (Carus, 2002). The five cases of bioterrorists Carus mentions are the Rajneeshees, Aum Shinrikyo, Dark Harvest, Mau Mau, and the Polish Resistance. The most prominent cases are the Rajneeshees and Aum Shinrikyo, which experienced the most success. To understand the roadblocks they nonetheless encountered, it is crucial to understand how these two organizations functioned and attempted to employ bioweapons.
Rajneeshees – In 1984, the Rajneeshees cult carried out one of the largest bioterrorist actions in U.S. History. Attempting to sway local elections in Oregon, they contaminated several restaurants with Salmonella typhimurium, which was responsible for infecting 751people with gastroenteritis (Carus, 2002). The Rajneeshees were originally an Indian cult that moved to Oregon to distance itself from notoriety in India. Upon settling in Oregon, they had a fractured relationship with local inhabitants. The cult would routinely bring in homeless people from all over the country to vote in local elections, hoping to sway land laws in their favor.
After several defeated electoral attempts, two of the prominent female members, Sheela and Puja, began to consider the use of biological weapons as a means to alter voter turnout. Puja, a registered nurse nicknamed “Dr. Mengeles”, controlled the Rajneesh Foundation International medical facilities and pharmacy. While Puja considered many biological agents, she chose S. typhimurium, a strain of salmonella most commonly associated with food poisoning. Other cult members stated that she also considered more severe bioweapons like HIV and giardia (Carus, 2002). Having purchased S. typhimurium from a commercial supplier, the Rajneeshees were able to produce more in covert laboratories within the Rajneeshees town, Rajneeshpuram.
Puja field-tested the pathogen on August 29, 1984 by contaminating the water of three county commissioners, all of whom fell ill. A second field test involved an unknown liquid that Puja employed cult members to spread on doorknobs and handles, but no infections were noted to occur. During August of 1984, the cult attempted several times to contaminate the water system, however, none were successful. In early September of 1984, the Rajneeshees poured vials containing S. typhimurium into different restaurant foods throughout their targeted town, The Dalles. The CDC estimates that 751 people became ill after eating at salad bars within these restaurants (Carus, 2002).
The Rajneeshees salmonella outbreak is considered by the FBI to be the only confirmed case of bioterrorism by a terrorist group operating in the U.S. until the 2001 Amerithrax attack (Carus, 2002). The uniqueness of this case is that it went unknown as an intentional outbreak. Even after wide public attention, this outbreak was not associated with bioterrorism until late 1985, when Rajneesh, the cult leader, emerged and stated he believed Sheela and 19 other leaders (including Puja) were responsible for crimes including the salmonella outbreak (Carus, 2002). Indeed, food terrorism is perhaps the most difficult form of bioterrorism to identify as intentional, as the pathogens are commonly occurring and biocrimes can easily be masked as large outbreaks. Overall, the Rajneeshees salmonella event is considered to be one of the largest case studies in biocrime history. Prior to the Amerithrax attacks, “this was the only confirmed instance of chemical or biological terrorism to occur in the U.S., according to the FBI” (Carus, 2002).
Aum Shinrikyo – Aum Shinrikyo was a Japanese group that is most famous for their release of sarin nerve gas in the Tokyo subway system. While this attack made them famous, few know that sarin gas was just one of dozens of chemical and biological weapons they were developing. From 1990 to 1995, Aum Shinrikyo worked to develop biological agents to support their apocalyptic religious goals. Believing that war with the U.S. was imminent, the cult felt that arming themselves with bioweapons would provide better protection. The leader, Asahara, was a highly charismatic man, establishing a cult of roughly 40,000 members worldwide. Many members were wealthy citizens and included several scientists and engineers. It is estimated that at their peak in 1995, Aum had roughly $1 billion in net worth, making it one of the most well funded terrorist groups (Tucker, 2000). The Armageddon mentality further pushed the group to develop weapons at a rapid pace, with an increasingly violent attitude as a result of growing paranoia they became increasingly dependent on narcotics.
Aum’s use of bioweapons started in 1990, with their attempts to develop the botulinum toxin that could be used to infect state officials and others they deemed enemies. Aum had a substantial research facility, allowing them to perform advanced microbiology and even to disseminate biological materials from the roof of the facility they owned. During this time period, they worked on botulinum toxins, Bacillus anthracis, and Ebola. Ebola is considered one of the world’s deadliest viruses and was such a prize item for Aum that members traveled to Zaire in 1992 on a “humanitarian mission” during a local outbreak to supposedly acquire the virus in the wild (Thompson, 2006).
While they did extensive research, Aum actually made several attempts to field test and attack enemies with their manufactured weapons. In April 1990, they attempted to disseminate botulinum toxin by spraying the toxins from three vehicles when driving through central Tokyo, one of the international airports, and a naval base (Thompson, 2006). In 1993, they also tried the drive-by method at a royal wedding in Tokyo (Carus, 2002). Later that year, they attempted to spread anthrax using a sprayer system on the roof of a building they owned, as well as trying to contaminate the area around the Diet using the similar truck methods (Carus, 2002). The truck drive-by method was also employed again in mid 1993 during an attempted attack around the Imperial Palace in Tokyo (Carus, 2002). Lastly, in March 1995, Aum planted three briefcases in the Tokyo subway to release botulism. Interestingly, the individual responsible for preparing the suitcases had moral trepidation and replaced the contents with a placebo (Thompson, 2006).
This particular failure pushed Aum to use sarin nerve gas, which is not a bioweapon but a chemical warfare agent (Carus, 2002). The 1995 sarin attack was carried out in morning rush hour by placing the liquid sarin in punctured packages that looked like bottled drinks onto five cars, across three separate subway lines. The sarin attack was deemed successful by Aum, as it killed 12 people and caused over 6,000 to seek medical attention (Fletcher, 2012). Despite all of these bioweapon attempts (10 in total), they were all met with failures (Tucker, 2000). The sarin nerve gas attack was their only source of success, pointing to the unanticipated difficult nature of bioterrorism. Whether the result was a failure of dissemination, the virulence of the pathogen, or internal collapse within the group, Aum is a prime example of the dedication some organizations have to employing bioweapons, but also the roadblocks that prevented their success. Despite the resources Aum Shinrikyo had, in most cases they were unable to effectively use biological agents.
Amerithrax Attacks of 2001– After the terrorist attacks on September 11, 2001, letters containing anthrax spores were sent through the United States Postal System (USPS). Coined the “Amerithrax” attacks, this case is noted to be the “worst biological attack in U.S. history” (FBI, n.d.). An estimated 10,000 people were exposed and 22 people experienced illness, of which five died. Anthrax is an extremely potent pathogen when inhaled, and with approximately 20 billion total spores released in the letters, this attack cost an estimated $6 billion in response measures (Thompson, 2006). Bacillus anthracis exists in roughly 89 known strains, but this particular strain was known as Ames (Thompson, 2006). What is unique about the Ames strain is that it is naturally occurring the U.S. (originally isolated in Ames, Iowa), highly virulent, and very resistant to existing vaccines.
From the beginning, the perpetrator was suspected to be an adult male who worked in a laboratory or had extensive scientific experience. Barbara Rosenberg of the Federation of American Scientists (FAS), who works on biological weapons, “believes the individual to be an American scientist with access to anthrax or at least instructed to make it by an expert” (Thompson, 2006). Dr. Rosenberg, as Thompson noted, “falls into what some call the ‘Bioevangelist Camp’, believing an American scientist with experience in the realm of bioweapons thought the U.S. was failing to give BW risk adequate attention. The attacker demonstrated bioterrorism’s potential and blamed it on a large threat – Al Qaeda. The scientist brought attention to the problem, finally summoning sufficient assets to focus on the issue” (Thompson, 2006).
Richard Spertzel, a researcher working on bioweapons at Fort Detrick, Maryland, and Head of the Biological Weapons Inspections from 1994 to 1998, testified to the House Committee on International Relations in 2001 that the anthrax used in these attacks had to have been produced by a non-state group with ties to a state-sponsored weapons program. He stated that the complexity of the attack pointed to a pathogen that was at least as pure and concentrated as those found in state bioweapons programs, specifically the U.S., Soviet, or Iraqi programs (Thompson, 2006). The largest source of the Ames strand in the U.S. is found in the United States Army Military Institute for Infectious Diseases (USAMRIID).
While the culprit in the Amerithrax attack is still unknown, in 2008 the Department of Justice and the FBI brought charges against Dr. Bruce Ivins. Despite his suicide in 2008, evidence continues to mount against Dr. Ivins. A biodefense expert whose personal emails stated his willingness to hurt, kill, and terrorize, he was a microbiologist who worked with anthrax for decades at USAMRIID (Shane, 2010). Dr. Ivins was specifically working on vaccines for anthrax, revealing his extensive knowledge and access to the pathogen. While the Amerithrax attack does not have an obvious terrorist culprit and motive like those by Aum Shinrikyo or Rajneeshees, it continues to worry biodefense experts regarding apparent U.S. vulnerability.
Additional cases – There are three additional cases that are worth mentioning, but not heavily analyzed as there is little evidence available (Carus, 2002). Dark Harvest was a group that protested anthrax military testing by the British military during WWII and attempted to contaminate research facilities with anthrax-contaminated soil. Studies revealed that the soil had low levels of anthrax spores that were unable to cause illness. The Mau Mau African independence movement group was believed to be responsible for poisoning livestock with a plant toxin, but little information is available. Lastly, there are reports that during WWII, Polish resistance organizations used biological weapons to produce a claimed 200 German deaths.
METHODOLOGY
Case Selection
The cases addressed in this thesis reflect those that have substantial data and background information to truly determine hurdles encountered in bioweapon utilization. The primary cases for discussion are the Aum Shinrikyo attacks from 1990-1995 and those by the Rajneeshees cult. While this thesis will refer to other non-state terrorist organization attempts, there is insufficient evidence that they represent actual attempts to use bioweapons. Carus categorizes cases according to terrorist, criminal, or other purposes.
For the rationale of this analysis, attention will be spent on the terrorist activity involving bioweapons. While criminals can be considered non-state actors, the cases associated with such action typically involve small clusters of poisoning (for example, employees poisoning doughnuts to infect coworkers and spouses infecting in-laws) and are not deemed terrorist incidents. According to Carus, motives of criminal cases were narrow and primarily involved targeting individuals or extremely small groups, not on instigating fear or social disruption on a large scale. The Amerithrax attacks will not be as heavily analyzed as those of Aum and Rajneeshees. The reasoning for this general exclusion is the debated classification of the Amerithrax attacks as truly terrorist attacks. Carus’s 2002 assessment does not include the Amerithrax attacks, most likely a result of the limited information at the time of print, and its classification as a terrorist action is disputed (Carus, 2002).
Many in the scientific community believe that the lone-wolf nature of the Amerithrax attacks and general intent behind them do not match terrorist habits (Thompson, 2006; Leitenberg, 2006). While there are valid points to both sides, the attacks will be referenced, but the lack of information regarding the perpetrator and attack methodology is not conducive for this analysis. The discussion will include some general information regarding the complexity of the Amerithrax case, since despite its disputed motives, this biological attack is nonetheless considered the largest in U.S. history.
Analysis Criteria
The analysis of these cases, specifically the Aum and Rajneeshees attacks, focuses on 7 key roadblocks to successful use of biological weapons by terrorist groups:
- Accessibility/availability of the biological agent
- Difficulty of weaponizing
- Dissemination
- Environmental Conditions
- Communicability and Incubation Period
- Response Measures
- Attitude and Intent of Potential Users
While many studies have focused on vulnerability to bioweapons attack, this analysis will focus on the capabilities that non-state actors must possess to use bioterrorism. The capability criteria are derived from both commonalities between cases, knowledge of epidemiological factors and public health response capabilities, and existing literature on non-state actors and their consideration or use of bioweapons. Previous analyses, like those of Carus, Thompson, and Tucker, have been case specific, choosing to focus on the cases and then to identify the roadblocks. This analysis will, however, focus on the hurdles and their role in the attacks.
The majority of current literature also fails to point out the epidemiological components of these pathogens; from communicability to public health response, there is a general gap that this analysis hopes to fill. By focusing on threat, capabilities (ability or potential to develop and disseminate bioweapons), intent, and epidemiological components of bioweapons, this thesis will provide a capabilities assessment of previous bioattacks to understand why bioterrorism never reached heightened popularity.
Barriers for Utilization
ACCESSABILITY/AVAILABILITY OF AGENT
One of the technical hurdles in bioterrorism, after a group has decided upon that route, is to actually obtain the pathogen. Some non-state actors have been foolish in their approach to this technical hurdle. Aum Shinrikyo, for example, thought that they could acquire the live Ebola virus, considered to be one of the deadliest pathogens known to man, by traveling to Zaire during an outbreak. This was not a realistic approach, but there are several methods to acquiring a pathogen. The first involves purchasing the agent from a medical/microbiology supply company. The Rajneeshees actually purchased their salmonella cultures legally from the supplier, VWR Scientific, as well as several other pathogens from American Type Culture Collection (ATCC) (Tucker, 2000).
One of the most shocking aspects of the Rajneeshees investigation was that the purchase orders for such pathogens also revealed that they could order tularemia, shigella dysentery, and typhoid fever, which are all extremely dangerous bacteria (Thompson, 2006). The Minnesota Patriots Council, an anti-government activist group, was found to subscribe to a publication that held advertisements for “Silent Tool of Justice” kits that included “an inexpensive assassination kit based on ricin” (Tucker, 2000). Carus noted that of the 33 cases involving acquisition by non-state actors (including terrorists, criminals, and “others”), 11 obtained their pathogens from legitimate suppliers. The 11 cases included the acquisition of Y. pestis (plague), Clostridium botulinum, and Clostridium tetani.
The medical clinics and facilities that both Aum Shinrikyo and Ranjeeshees retained allowed them to legally acquire these pathogens, but smaller non-state actors, like Larry Wayne Harris (a Christian Identity Church member who purchased y. pestis and claimed he had possession of large quantities of anthrax), met with challenges when attempting to acquire these agents from culture collection companies (Tucker, 2000). Harris was actually able to obtain Y. petis and anthrax (the vaccine strain) through the ATCC, but only after substantial trouble. The ATCC told Harris that to order cultures and have an account, he had to run an established lab with a letterhead (Tucker, 2000). Harris was able to resolve this dilemma by going to a local print shop and having stationary made using a fake lab name and his home address (Tucker, 2000). Sadly, this worked. Legally acquiring agents has become more difficult since the Amerithrax attacks and the focus on bioweapon security, but there is still an obtainable capability to purchase these pathogens with an established laboratory account.
The second method of acquiring pathogens is through theft. Carus noted that four of the 33 cases of acquisition by non-state actors involved stealing a biological agent from a research or medical facility. Carus found that, “almost all of the thefts involved people who had legitimate access to the facilities where the biological agents were kept” (Carus, 2002). Several cases involved laboratory technicians, graduate students, or hospital staff stealing cultures. The anti-government group Weather Underground attempted to obtain agents by blackmailing soldiers at Fort Detrick, Maryland, however, this tactic was not successful. Cases of theft have been mostly by individuals or small groups, but most cases caught the attention of other lab technicians or coworkers, who alerted authorities. Fox noted that restrictions on microorganisms have greatly tightened since the Amerithrax attacks. He found that accessibility of many microorganisms has become stricter and the process for working with certain agents involves extensive reporting, review, and security (Fox, 2002).
Nonetheless, Malet found that while there was a rapid succession after Amerithrax to tighten pathogen security, the dual-use nature of biotechnology is a cause for significant concern and that “much of this work (civilian medical or agricultural technological development that can easily be adapted for bioweapon use) is conducted at least partially in the private and academic sectors without the full oversight of the government and there are already troubling indications for these developments to escape both oversight and the intent of the policymakers.” He also stated that the “current biodefense programs actually pose the greatest risk for the use of Weapons of Mass Destruction against the U.S. and deserve substantial reconsideration (Malet, 2010). These changes make legally and illegally acquiring pathogens considerably more difficult for non-state actors, especially those of smaller organizations that do not own medical facilities or that face tightened security measures in laboratories they were hoping to infiltrate.
The last acquisition method is through manufacturing the pathogen or isolating it from a naturally occurring reservoir. Of the 33 acquisitions on Carus’s list, 12 involved manufacturing the agent or acquiring it from a living host without any processing. Six of the 12 cases involved groups “building” their own pathogen. This method is really exclusive to toxins like C. botulinum (botulism) and ricin from castor beans. It is not possible to manufacture a virus or bacteria, but one can produce toxins from manuals like the Poisoner’s Handbook, Silent Death, Catalogue of Silent Tools of Justice, and the Anarchist’s Cookbook. Manufacturing these toxins, especially ricin, is extremely dangerous, and if done by an inexperienced person who is not extremely careful, can lead to death. There have been cases in Maricopa County, Arizona, where people attempting to make ricin caused extreme chemical reactions leading to property damage or death (Evans, 2013).
Another method for obtaining a pathogen “naturally” is by acquiring it from its natural source, i.e. an infected host. This specific method does not involve any processing, but rather extracting blood or other potentially infectious materials from an infected source and directly infecting a person. Natural acquisitions from animal or human hosts also account for 6 of the 12 cases identified by Carus as manufacturing or natural source acquisitions (out of 33 total cases of groups actually acquiring the agent).
Some simple attempts involved using a whole castor bean (with no manufacturing to isolate the toxin) as means to poison a person. Most of these cases involved individuals injecting HIV infected blood into a victim. Rajneeshees member Puja was suspected of injecting a fellow cult member with HIV, but it was never proven. This was also the intent of Aum Shinrikyo when they traveled to Zaire in hopes of acquiring the Ebola virus from a living host (Thompson, 2006; Carus, 2002). This method has also been used to isolate anthrax from soil, as it is naturally occurring. Many have considered isolating Y. pestis from prairie dogs or other hosts in endemic regions (Leard, 2013). States like Arizona are habitats for animals like prairie dogs that carry the infected fleas, which cause plague cases.
Overall, acquiring these agents, whether through purchase, theft, or manufacturing via a natural source, has inherent risk and requires both technical knowledge and connections. Obtaining an agent is not enough, but rather the non-state actor must have the medical facilities and laboratory to house and work on the pathogen. Even if one has access to their own facility and has extensively trained technicians or pathologists, the access to these agents has reportedly become increasingly tightened, making it far more difficult for individuals or groups to acquire them. Nordmann pointed to the recommendations made by the 2008 Commission on the Prevention of Weapons of Mass Destruction Proliferation and Terrorism to increase biosecurity, but the reality is that these measures could take time to be enacted (Nordmann, 2010). Nonetheless, there is a substantial push to make biosecurity measures more secure and universal. Although this initial roadblock is currently most likely one of the easiest to overcome, as time progresses and the concern for bioterrorism grows, restrictions will also tighten on legally purchasing these organisms and on access to facilities that house them. The only alternatives will increasingly be to acquire them naturally, which is extremely technically intensive and demanding.
Monetary Deterrents
Beyond the accessibility and availability of biological agents is the hurdle of having financial means to acquire them. Aum Shinrikyo had considerable options, as they were one of the most well funded terrorist organizations. With roughly $1 billion in funds, they owned several buildings, including hidden medical facilities, and were able to fund bioweapon trials (Thompson, 2006). While individuals like Larry Wayne Harris were able to pay for these organisms online, the availability of these pathogens has been regulated in recent years to prevent such events from occurring (Tucker, 2000). Acquiring an agent via theft can also be monetarily taxing, as bribes and the equipment to transport the pathogen could be costly. Attempting to isolate a pathogen naturally is also extremely expensive, requiring all the necessary laboratory equipment, which in the case of viruses, is extensive. Beyond the technical know-how needed for this method, the purchasing of the equipment alone is a major deterrent. One can not simply collect dirt and isolate anthrax.
WEAPONIZING THE AGENT
Viability of the Pathogen
Once a non-state actor has made it past the first hurdle and acquired an agent, the real work begins. Weaponizing an agent through cultivation (the process of growing biological pathogens) and dissemination (spreading the pathogen to individuals for disease transmission) are two of the most technically demanding and failure-prone components of bioterrorism. While terrorists with financial resources can gain access to laboratory equipment for weaponizing, as it is technically “dual-use”, this does not guarantee proficiency using it. Dual use refers to the fact that the equipment needed for creating bioweapons is the same equipment needed to help isolate pathogens for vaccine or treatment research. Figure 3 provides a clear view of how dual use can work to the bioterrorist’s advantage (Thompson, 2006). All the laboratory equipment is commercially available, albeit pricey. After purchasing the equipment (glassware, desktop fermenter, and standard nutrient media) and obtaining the pathogen, the ability to isolate and grow the pathogen comes into play. Viruses are the most difficult in that they cannot live outside a living cell, but require fertilized eggs in which to grow. Just as Aum Shinrikyo attempted to isolate toxin strains of botulism from soil, they ran into the necessity for technical knowledge needed to isolate large quantities via enrichment materials (Thompson, 2006; Tucker, 2000).
Purifying toxins is especially difficult. Rosenau noted that, “botulinum toxins are extremely difficult to purify, particularly in large quantities, and are highly unstable in pure from. Purification entails the separation of the toxin from the cells that create it. The difficulty of producing a sufficiently pure toxin is compounded by the fact that the protein-destroying enzyme is generated at the same time as the toxin. Maintaining the toxicity of the material as it is purified is extremely difficult” (Rosenau, 2001). U.S. government researchers have found that attempts to reach 95% purity (the level to truly cause mass illness) reduces the amount of the toxin to 70-80% (Rosenau, 2001). Toxins especially degrade quickly when exposed to sunlight and air, which means they can lose their efficacy by a rate of 4% per minute (Rosenau, 2001).
The same issue also arises when attempting to isolate a toxic form of anthrax. Anthrax is naturally occurring in soil and does not cause illness (except in livestock and rare cases of humans), but isolating and transforming specific B. anthracis dormant spores into active, aerosolized particles is technically very complex (Zubay, 2005). The spore itself is highly resistant to environmental stresses but is also very unstable in its vegetative state, which requires extensive microbiological knowledge and experience to cultivate spores and not kill them when they are in the vegetative state. Attempts to isolate and grow B. anthracis are also compounded by the knowledge needed to identify the correct strain (Rosenau, 2001; Zubay, 2005). There are several bacillus species, but identifying and growing the correct one requires years of knowledge. Once the correct bacteria is isolated, awaking it from the dormant state becomes progressively challenging, as it requires heat or chemical shock without killing the pathogen (Zubay, 2005; Roseanu, 2001).
Bacteria are probably the easiest of the pathogens to isolate and cultivate, but viruses are considerably more difficult. Both Rajneeshees and Aum Shinrikyo had considered obtaining and utilizing viruses like Ebola (a viral hemorrhagic fever) and HIV (Carus, 2002; Tucker, 2000). Viruses like those that appeal to terrorists are extremely difficult to isolate and grow, as the required host cells must be living. Consider the weaponization of influenza, which is easier to obtain naturally than any other category A or B agent.
Viruses may require genetic engineering, which becomes considerably more taxing on both technical knowledge and equipment. Influenza, while a naturally occurring virus, frequently mutates or has antigenic drifts, which is the reason for new flu vaccines every year. Antigenic shifts are major changes in the virus’s proteins, which make novel influenzas a risk for pandemics, as there is no immunity to such massive gene segment changes. Zubay has noted that, “key characteristics of good bioterrorist weapons are ease of production and ease of obtaining the pathogens” (Zubay, 2006). Ironically, of all the prospected viruses, influenza meets this criteria. However, it has not been utilized like bacteria as a bioweapon, which may reflect substantial specialized knowledge needed for such a task.
The technical hurdles associated with pathogen cultivation make this one of the greatest roadblocks for non-state actors with limited resources, technical knowledge, and temporal restrictions. Aum Shinrikyo spent years working on weaponizing their agents, which began to erode morale, monetary resources, and interest in bioterrorism. (Tucker, 2000). Enemark pointed out that, “it is simply not enough to be able to grow a biological agent that makes people sick. In addition, the agent must be kept alive, it must be of a strain that is lethal to humans” (Enemark, 2006).
Professional Expertise
The technical knowledge and experience necessary for isolating, cultivating, and weaponizing pathogens for bioweapons is a particular hurdle that has prevented several terrorist organizations from being successful. Given the technical difficulty in housing, cultivating, and weaponizing an agent, the need for persons trained in virology, pathology, or microbiology is crucial. The mental degradation of Aum Shinrikyo members through drug use and paranoia is suggested to have severely reduced their ability continue such technically proficient work (Tucker, 2000). While drug use and paranoia was rampant in Aum, these matters were coupled with general technical hurdles that required substantial scientific experience to solve the issues. Aum’s head microbiologist and bioweapons specialist, Seiichi Endo, was unable to cultivate a lethal strain of botulism, which most likely was a result of his inexperience in microbiology (Rosenau, 2001). Endo was trained as a molecular biologist, not a microbiologist, so as their head of bioweapons he significantly lacked the necessary technical expertise.
The Amerithrax attacks highlight the extensive expertise that is needed for large-scale, complex biological attacks. Anthrax, as previously discussed, is extremely volatile and difficult to weaponize, which is why the suspect was believed to be an extremely experienced microbiologist with years of experience not just in the field, but also with that particular organism. Acquiring a lethal strain of anthrax or botulinum is especially difficult as there are several strains that can be harmless. Only an experienced researcher or laboratory microbiologist would know how to isolate and cultivate the lethal strains. The Rajneeshees were able to easily acquire S. typhirium (arriving on bactrol disks) and grow the bacteria in larger quantities as a result of an experienced laboratory technician who also manufactured it into liquid form (Carus, 2002). The ability to transfer and grow bacteria, especially salmonella, is far easier than that of botulinum or anthrax, but still requires a basic understanding of the laboratory practices.
Knowledge and skills to use the equipment is also a considerable hurdle. Laboratory equipment, especially that needed to isolate and weaponize mass quantities of bacteria or virus, is extremely complex and can be dangerous. Equipment misuse or poor technique can be devastating to the individual working on the experiment. Tucker found that “because of sloppy laboratory practices, members of the Aum Shinrikyo cult reportedly became infected with Q-fever, a rickettsial disease they were prepping as a biological weapon. Even cult leader Shoko Asahara is believed to have acquired the debilitating illness” (Tucker, 2000).
DISSEMINATION
Dissemination is considered to be the greatest of hurdles in bioterrorism. Tucker has noted that although “persistent chemical agents such as sulfur mustard and VX nerve gas are readily absorbed through the intact skin, no bacteria or viruses can enter the body by any route unless the skin is already broken. Thus, BW agents must either be ingested or inhaled to cause infection” (Tucker, 2000). A biological weapon must have a means of transmission, and to be effective, this transmission should reach as many people as possible.
Aerosolization
There are several routes of dissemination, but the one most attempted and of most concern to biosecurity experts is aerosolization. Aerosolization is a means of creating a cloud that contains the infectious agents via microscopic droplets for victims to inhale. Respiratory inhalation is the most dangerous form for both plague and anthrax, which underscores the appeal that aerosolization has for terrorists. Aerosolization also has the capacity to infect large numbers of people over substantial geographical spaces. Calculations found that 100 kilograms of anthrax spread over Washington, D.C., could kill 1-3 million people, versus a one-megaton nuclear warhead, which would kill a maximum of 1.9 million (Carus, 2002).
The Amerithrax attacks were a good example of aerosolization in the most rudimentary, non-technical delivery form. The perpetrator did not develop an aerosolization method, but rather the spores were so finely prepared that they easily traveled in the air. While this route of dissemination is the most appealing, it also had the largest technical hurdles. For effective inhalation, the particles in an aerosol cloud have to be roughly 1-5 microns (one-millionth of a meter) in size (Carus, 2002). Particles larger than 5 microns will be caught through the respiratory tract filter and often are too heavy to travel, thus they fall quickly and are not as effective voyagers. Aum Shinrikyo is one particular group that attempted to use aerosolization in the truest technical form (Carus, 2002). By developing delivery systems like sprayers that aerosolize pathogens into a cloud, terrorists can discretely release large amounts of bioweapons into a wide geographical area.
Aerosolization, however, is an extremely complicated process. To spread an agent through the air, it must be in either liquid (slurry) or dry form, which in and of itself is an arduous task. Those preparing it must then address both physical issues (to ensure the sprayer nozzles do not become clogged) and biological issues (to ensure that the organisms can survive once aerosolized). An agent in liquid form can be aerosolized using a modified commercially available sprayer, but problems remain. Most agents die in the spraying process- estimates range as high as 99% (Rosenau, 2001). “In contrast, a dry agent is relatively simple to disseminate, but most experts agree producing it is a dangerous process almost certainly beyond the capabilities of non-state actors” (Carus, 2002). Rosenau also noted that to truly cause massive casualties, an aerosolized cloud, not just sprayed material (like Windex), is needed (Rosenau, 2001).
The slurry form of a pathogen can quickly clog spraying canisters or fall to the bottom of the container, rendering it ineffective. Aum Shinrikyo experienced this with their attempts to spread what they believed to be B. anthracis from a rooftop building in Tokyo. The bacteria slurry, which was actually a harmless anthrax strain, was not refrigerated until the very last minute, so the slurry settled at the bottom (Tucker, 2000). A pathogen in liquid or slurry state is also more difficult to aerosolize, as its size is larger, so it tends to fall more quickly. Rosenau also noted that bacteria tend to die more quickly in a slurry form as they are aerosolized (Rosenau, 2001). Perhaps one of the biggest issues with aerosolization is the fact that the pathogens tend to lose their toxicity not only in the aerosolization process, but also as they enter the atmosphere. Environmental conditions, which will be discussed later, pose serious risks to the viability of pathogens.
Overall, aerosolization is the most effective dissemination strategy, but also has the largest number of complications. Aerosolization, while the most appealing as it can lead to higher efficacy if done correctly, poses the largest amount of technical obstacles for non-state actors to overcome. The delivery system requires substantial technological prowess, but also the form of the pathogen can alter the efficacy of the aerosolization. Dry or slurry format can create problems in the actual delivery device, as well as efficacy for the pathogen to stay within 1-5 microns in size and travel considerable distances.
Food & Water Contamination
Food terrorism and water contamination are also often considered or used by terrorists to disseminate pathogens. The potentially far-reaching implications for a massive food or water supply contamination could be just as considerable as for aerosolization if done on a large-scale basis. Intentional food and water contamination is extremely difficult on a large-scale, however, it incapacitates victims rather than killing them, meaning that for terrorists it has costs that potentially outweigh the benefits when compared to other dissemination methods.
While there has been, according to Carus, no known terrorist attack upon a water supply, many groups like the Green R.I.S.E and the Weathermen organization planned to dump pathogens into large water supplies (Carus, 2000). The Rajneeshees also attempted to infect several water supplies in Oregon, but were unable to as a result of security measures (Thompson, 2006). The difficulty in waterborne distribution is that the agent must be able to survive in water (despite chlorination and other treatments), have relatively high virulence (be able to cause illness with few particles, versus thousands, as it will be diluted in large water supplies), and be undetectable by water filtration systems.
Modern sanitation and food processing practices (such as pasteurization, boiling and cooking) would render most agents useless. Large-scale attacks using water supplies would be extremely difficult as the organisms would be highly diluted and picked up via filtration and treatment processes. Also, municipal water centers have security in place, which may deter potential terrorists. Organisms like Cryptosporidiosis (a protozoa very resistant to chlorine), giardiasis (protozoa found in untreated water), Vibrio choloerae (cholera), Shigella dysenteriae (dysentery), and Legionalla pneumophila (legionellosis) are all common waterborne diseases that are monitored (Heymann, 2008). The distinctiveness of waterborne or foodborne attacks is that they naturally occur and tend to go unnoticed as intentional, which may run counter to the terrorist organization’s goals.
Food is also a potential medium of dissemination. This approach has the most cases of illness associated with it as a result of the Rajneeshees attack in Oregon, which sickened 751 people. Contamination of the salad bars by the cult went unnoticed by officials as intentional contamination, which again may run counter to organizational goals (if the organization wishes to acquire media attention, unlike the Rajneeshees, which remained anonymous). Food terrorism (or agroterrorism involving the contamination of crops or livestock) on a large scale is labor intensive, as the pathogens have to essentially reach food at the production or distribution level and survive long enough to infect people.
While this is a major concern for the U.S., the organisms that can be used in food, aside from C. botulinum, are more debilitating than deadly. In the Rajneeshees case, they needed to sicken thousands of people to alter voter turnout, but were able to infect only 751 victims, which cost them considerable monetary funds, manpower, and technical expertise. In many ways, food terrorism, to be truly effective, requires a massive undertaking that still does not have as much potential impact as an aerosolization attack.
Suicide Cases
The use of an infected individual as a suicide bomb has not yet been utilized, but still demands attention. Just like suicide bombers, the idea of intentionally infecting a non-state actor organization’s member with a highly infectious pathogen has been discussed by biodefense experts and public health response modelers (Tucker, 2000). Glamorized in films (Contagion, Twelve Monkeys, and the television show Body of Evidence), such an attack in reality is far more difficult to accomplish. Firstly, suicide bombers suffer a quick death, while suicide bioterrorists will slowly and perhaps painfully die of infection, which may dissuade potential users.
The pathogens that are most applicable for this dissemination method are the highly infectious ones like smallpox, pneumonic plague, and viral hemorrhagic fevers. The hurdles regarding these organisms are both acquisition and incapacitation of the host. Smallpox has been vaccinated against to the point where the last natural case was in 1949 in the U.S. and 1977 worldwide (Zubay, 2005). Smallpox has been such a source of concern that despite the virus only being kept in 3 secure locations, scientists have annually pushed for the remaining strains to be killed (Preston, 2003). Viral hemorrhagic fevers occur sporadically, mostly in Africa, and have technical issues as the person would either have to directly infect themselves via a sick person during an outbreak and only have a few days before the onset of symptoms, or secure a sample and wait to induce infection for a more suitable moment. Enemark has noted that even if the population is susceptible (not vaccinated), a few cases may not be enough to cause an epidemic (Enemark, 2006). The biggest roadblock with suicide bioterrorism is the incubation period and eventual incapacitation of the “bomber”, which would greatly diminish efficacy if not calculated properly.
Capabilities Assessment
Dissemination capabilities pose the greatest hurdle when attempting bioterrorism. All of the dissemination methods require certain capabilities to be successful. Complex pathogens not only pose difficulties during the acquisition and weaponization stages, but also pose toxicity issues during dissemination. The most effective but technically challenging dissemination approach would be aerosolization, and the attempts made by Aum Shinrikyo point to the complexity and susceptibility to failure that this method poses. Food contamination by the Rajneeshees cult was the most effective, most likely as a result of the simplicity of the pathogen chosen and the route utilized. In terms of dissemination, it seems that the more rudimentary the method, the more successful it is in terms of disease transmission. The Amerithrax attacks are unique in their sophistication. The dissemination route was dependent upon the pathogen’s capabilities, which only highly experienced microbiologists could achieve. The aptitude for a non-state actor to stick to more basic organisms and dissemination methods when there is limited technical expertise provides a higher rate of success.
ENVIRONMENTAL CONDITIONS
Environmental conditions like sunlight, rain, humidity, temperature, wind, and altitude clearly impact the efficacy of a bioterrorism attempt. Microorganisms are uniquely susceptible to environmental degradation, which makes this component an especially difficult hurdle to account for when planning an attack.
Wind
Environmental and meteorological conditions are surprisingly a large component of the successful bioterrorism attacks. Wind speeds and direction present a serious hurdle for aerosolization attempts. Environmental conditions, specifically wind, create large variation in outcomes, which could defeat the organization pursing them. Aerosolization is the most effective method of dissemination, but beyond its technical hurdles, it is also the most susceptible to environmental conditions. Particles must be between 1-5 microns for effective inhalation and aerosolization devices. Wind can carry pathogen particles far distances, but it can also greatly diminish the efficacy of dissemination. Rosenau has noted that, “if wind speed is less than 5 mph, the aerosol will be limited in coverage. If wind speed exceeds 30 mph the aerosol disintegrates, loses its integrity, and effects on the target cannot be predicted” (Rosenau, 2001).
Wind was a particular issue for Aum Shinrikyo’s attempt to release anthrax from a building rooftop in downtown Tokyo. Their aerosolization attempts were usually from high buildings during the summer months with little wind, strong sunlight, and high amounts of smog and rain (Rosenau, 2001). The role of environmental conditions was further reinforced by the success of their sarin attacks, which were in confined areas with small bursts of wind from subways. Tucker also notes that only under the most stable atmospheric conditions do aerosol clouds stay close to the ground, where they can be dispersed and inhaled (Tucker, 2000). There is also concern that wind direction may pose risks for the terrorist group. If specific populations (such as stadiums and public gatherings) are the target, then a change in wind direction could put not only the organization at risk, but also untargeted persons.
Heat & Humidity
Heat, moisture, and precipitation can also severely impact the ability to release a pathogen into the environment. Most agents are extremely vulnerable to sunlight and heat. Biological agents released in the day, like those used by Aum Shinrikyo, have significantly higher failure rates. UV radiation is a significant vulnerability for microorganisms, with many unable to survive longer than 30 minutes in sunlight. While anthrax is able to survive these tough conditions as a result of its induced spore form, humidity in the air may hinder its ability to disperse (Tucker, 2000). Rainy seasons and environments with relative high humidity levels can prevent microorganisms from aerosolizing.
Recent studies analyzing the role of humidity and temperature on the transmission of influenza found that relative humidity (RH) levels played a large role. In high RH (80%), influenza droplets settle too rapidly, making aerosolized transmission exceedingly difficult. Aerosolized transmission was highest at low RH (20-35%) and at some higher RH levels (65%), but not beyond 80%. The lowest transmission occurred at medium and extremely high RH levels. The study also found that transmission efficacy was inversely correlated with temperature. Lower temperatures (5°C) permitted a statistically significant higher rate of transmission compared to 20 °C (Lowen, 2007). Given the role of humidity and temperature on pathogen survival and aerosolized transmission, finding conducive environmental conditions may be exceedingly difficult.
Altitude of Dissemination
Altitude draws upon all of the aforementioned environmental conditions. As Aum Shinrikyo found through their rooftop dissemination attempt, locations too high may face wind, rain, and smog conditions that render these attempts useless. The oxygen levels of high altitude conditions can also increase the rate of microbial decay, as some bacteria are aerobic, meaning they require oxygen. The biggest concern with high-altitude dissemination attempts is the role of wind and geographical distance. Wind changes can alter the course of pathogen distribution, but also inhibit its spread. Higher altitude locations will have higher wind speeds, which will break down the aerosol’s integrity. Aum Shinrikyo thought that a higher building would equate to a larger geographical distribution, however, it also heavily contributed to their failure (Thompson, 2006; Rosenau, 2001).
COMMUNICABILITY AND INCUBATION PERIOD
Communicability and RO
Disease transmission is heavily reliant on communicability, which is the ability for a pathogen to be spread from person to person. Pathogens can spread from person to person (contact, droplet, and aerosol for influenza, tuberculosis, salmonella), from vector to human (mosquitos and tics for the West Nile virus, and the plague), and zoonotic routes (from animals through ingestion or exposure, such as for Ebola, rabies). Person-to-person contact can happen directly or indirectly. Direct contact would occur via such things as a sneeze or cough, while indirect contact would involve a fomite (intimate object) like a counter top or doorknob.
A key component of infectious disease epidemiology is the reproductive number, R or Ro, which points to how many secondary cases a primary case will cause. Epidemics can be predicted by Ro, as these numbers will dictate the ability for an infected person to spread the disease. Ro is calculated by the infectiveness of the person, susceptible population, and attack rate (Kramer, 2010). If Ro <1, the infection will die out, but if Ro >1, then it can easily spread through a population. The larger the value of Ro, the potentially larger the epidemic is and the more difficult it is to control. Common Ro values are 12-18 for measles, 5-7 for smallpox, 2-3 for influenza, and 2-5 for HIV/AIDS.
The communicability and Ro of a pathogen greatly determines its longevity as a bioweapon. Pathogens like smallpox and plague have higher Ro and are more communicable than botulism and anthrax. Person-to-person transmission of inhalation anthrax does not occur; rather, spores fly off clothing or become aerosolized through movement. Botulism is the same, as it requires ingesting the toxin. Figure 6 displays the communicability of the Category A agents. Interestingly, the pathogens most commonly used in bioterrorism attempts are those that have extremely low Ro. Pneumonic plague, viral hemorrhagic fevers, and smallpox are all much more communicable, and yet have limited reported use in biocrime history (Heymann, 2008; Tucker, 2000).
The communicability of bioweapons also poses trade-offs for terrorist groups. Agents with high Ro pose a risk to both the organization and non-targeted populations, while those with no communicability between people have short outbreak spans and limited target capacity. Communicable diseases are exceedingly hard to contain, and if a group is seeking to target a specific population, it would be nearly impossible to prevent unintentional secondary cases. Even for apocalyptic groups, the risk of infection among members may be deemed unnecessarily high. The communicability of pathogens is greatly variable, which can create high amounts of instability and discomfort in groups considering this route. Overall, these considerations may help explain a terrorist group’s reported pursuit and use of organisms with low or virtually no communicability.
Incubation Period
The time from exposure to infection and communicability may pose another roadblock for terrorists. This epidemiological obstacle for bioweapons has not been heavily researched, but several terrorist groups have reportedly encountered it. Incubation periods can range from hours to weeks depending upon the organism. Incubation periods of diseases are variable and dependent upon the type of exposure (inhalation, bloodborne, or mucous membrane) the organism itself, susceptibility of the host, and the target’s physiological conditions, all of which cannot be accounted for by a non-state actor.
There are several stages to infection, but as seen in Figure 4, there can be considerable time between exposure, incubation, and symptoms (Symptoms, n.d.). Toxins, like botulism, can cause illness in a matter of hours, while viruses tend to take longer.
Incubation periods represent a roadblock for bioterrorism because they have relatively large ranges and are difficult to predict. The Rajneeshees found this to be a problem, as they needed to infect a large group of the county population to prevent them from voting (Thompson, 2006). S. typhimurium did not just infect and incapacitate people all on one day, but rather over the course of roughly a week (Carus, 2002). If the intention of the attack is to cause illness during a certain time window, incubation periods can seriously erode the efficacy of such an attack. Incubation periods can also allow for pathogen identification and for treatment to be initiated before some of the exposed population is sickened. In the Amerithrax attacks, some individuals were sick before others, which triggered an investigation and allowed for an outbreak investigation to follow up with all exposed persons and initiate treatment (Preston, 2003; Thompson, 2006).
Incapacitation of Host
Each pathogen attacks its host in a unique manner, which contributes to bioweapons’ instability as an effective tool of terrorism. Stern noted that “terrorists want a lot of people watching, not a lot of people dead” (Stern, 2000). If the intention is to scare but not kill people, selection of the pathogen is crucial. Organisms like those of the Category A agents have the capacity to kill at high rates, while those like salmonella and influenza are largely incapacitating. If the terrorist’s goal is to instill fear and cause social and economic disruption, pathogens that cause illness and place a burden on health systems can achieve this.
Category A agents are more high-profile, but those like anthrax, which can quickly incapacitate and kill a patient, may run counter to the non-state actor’s intentions. Causing a large number of civilian deaths, for example, could create public anger against the terrorist group. If a person is infected with pneumonic plague or inhalation anthrax, they most likely will require extensive treatment in an intensive care unit (ICU), while someone infected with salmonella or influenza may not even be hospitalized. That is not to say that people infected with salmonella or influenza do not seek medical care or experience severe illness, but usually those that do are subsets of the population (elderly, children, and immunocompromised persons). The intensity of hospitalization and treatment is often a recognized assessment of the severity of the health condition.
RESPONSE MEASURES
Unusual or deadly pathogens raise a red flag in public health and healthcare, which triggers down-stream efforts to investigate and isolate. The U.S. public health system has surveillance and response protocols in place to identify and respond to cases of disease, whether endemic (naturally occurring) or epidemics (large cases of diseases beyond the normal case-load).
Surveillance
While most do not know the intricacies of its methods, disease surveillance provides a substantial strategy for diminishing the impact of bioterrorist events. Disease surveillance is the systematic collection and analysis of data to identify and monitor patterns within disease distribution. Public health is designed to provide disease surveillance and epidemiological response in cases of disease outbreaks. While not all countries have the same level of surveillance capability, governments, both nationally and through international agreements, have created public health organizations to prevent and control the spread of disease.
In the U.S., the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), and the Department of Health and Human Services (DHHS), work to provide public health support at a national level. Beyond these organizations, each U.S. state has a health department, as do their counties. Disease surveillance is performed either actively or passively. Active surveillance entails going out and collecting the information, while passive surveillance employs counterparts (such as hospitals, clinics, and universities) to collect data and pass it along. Most public health systems are passive unless there is an outbreak, mostly as a result of lack of resources. (Buehler, 2004).
Disease surveillance in the United States starts with a healthcare facility receiving a patient and obtaining labs or physician diagnosis that can confirm illness. Larger hospitals will have their own microbiology department that is capable of running extensive laboratory work from blood cultures to respiratory viral panels. State laboratories are commonly used for rare or complex tests that other facilities are unable to process. These tests tend to involve uncommon pathogens such as shiga-toxin producing Eschericia coli (the E.coli strain that was notorious for causing national outbreaks and associated deaths) and botulism. Once test results are reported, hospitals are required to report certain diseases to their county health departments. Each state has a list of “reportable communicable diseases” that range from anthrax, to plague, and syphilis (ADHS, n.d.).
Hospitals and state laboratories both report these cases with patient information to county health departments, who then report them to state health departments. Rare cases like measles or botulism would prompt communication with the CDC. Disease surveillance from specimen collection to county health department response can take a day in some cases. Specific diseases on reportable lists (those of the Category A, B, or C) require immediate phone calls, versus faxing or electronically reporting within a period of business days (ADHS, n.d.). Hospitals, state health departments, and county health departments all work very closely and in many cases are in communication on a daily basis.
Disease surveillance in the U.S. is taken very seriously at a health care level. It is very common for public health departments to do in-service education with emergency department physicians annually for training on uncommon diseases or “zebras”. After the Amerithrax attacks, there was a heightened awareness and education regarding bioweapon pathogens, so much so that physicians began to include them on differential diagnoses (initial triage diagnosis prior to any confirmatory lab work), which may have led to physician hypersensitivity regarding bioweapon issues.
There was a wave of eagerness to identify these pathogens after Amerithrax, leading to a hypersensitivity towards Category A agents (Cosgrove, 2005; Leitenberg, 2005). Jokingly coined “zebras”, these pathogens are rarely seen, but continuous education is provided to first responders. While there are gaps in any chain, the level of disease surveillance that occurs within the U.S. would very quickly pick up an usual agent and initiate response in a quick manner (NNDSS, n.d.).
This continuous education and reinforced disease reporting make it harder for bioweapons to go undetected. During large gatherings like sporting events and concerts, public health departments will touch base with health care facilities to remind them of the risk for outbreaks, and will perform active surveillance during the event. Syndromic surveillance has become increasingly common. This form of surveillance involves data collection regarding over-the-counter medications from drug stores, as well as emergency room visits involving chief complaints matching certain criteria (Henning, 20004). Syndromic surveillance uses logic-based software to detect large groups of people purchasing medication and/or seeking medical care for the same illness in a geographical area or time frame. There is also continuous development of more sensitive, real-time surveillance methods, which makes bioterrorism that much more difficult to carry out.
Identification
Once patients enter a healthcare facility, whether that of a primary care physician or a hospital emergency department, their symptoms are assessed and specimens are often taken. Since the Amerithrax attacks, several studies have addressed the knowledge gaps in the ability of physicians (especially emergency) to identify “zebras” or Category A agents (Cosgrove, 2005; Moye, 2007). As a result of these studies, extensive education has been enforced so that emergency and primary care physicians, as the first diagnosticians, would be able to more accurately identify or pick up on the symptoms associated with such illnesses. Physicians that see large patient populations are more exposed to a wide range of diseases, thus honing their diagnostic abilities. In areas where certain diseases are endemic (Y. pestis, plague, is endemic in states like Arizona and New Mexico, so physicians in these states are more familiar with the clinical signs and symptoms) or in patient populations where a disease occurs randomly (botulism in children or prisons), these diagnostic tools continuously are tested (Nania, 2013).
Overall, the gap in diagnostic capabilities has been identified and attention to bioterrorism and the commonly associated pathogens have been reinforced in the medical community. Healthcare workers from nurses to infection preventionists are educated at workshops and through federally funded training with the Department of Homeland Security Center for Domestic Preparedness (CDP), are better able to respond and handle epidemics and bioterrorism events (CDP, n.d.). Identification, while sensitive to human error, has become much stronger since the Amerithrax attacks, making bioterrorism a center stage topic for physicians. The increased education and capabilities to identify rare pathogens, especially those commonly used in bioterrorism, would likely prevent bioterrorism events from growing.
Treatment and Vaccination Measures
While many consider bioweapons to be unstoppable or without response measures, there are treatment methodologies in place to respond to their use. Vaccination and treatment techniques pose a severe hurdle for bioterrorists to overcome. For example, there are treatment protocols in place for all six Category A agents. Plague, anthrax, and tularemia are all treated with IV antibiotics, while botulism is treated with an antitoxin. Viral hemorrhagic fevers (VHF) are trickier: although Ribavirin, an antiviral, has shown efficacy against certain viruses, others can only be combatted with supportive care measures (Nania, September 2, 2013).
Smallpox is perhaps the most difficult, as there is currently no treatment for it, but immediate vaccination following exposure has been shown to be an effective response measure. Supportive care measures are also used in the case of smallpox. While smallpox and VHF may seem like effective bioweapons, they present difficulties. Both agents are viruses, making them difficult to handle and weaponize, and more importantly, both are extremely rare. No documented cases of smallpox have occurred in almost 40 years, and VHF occurs infrequently through small outbreaks in Africa. These two pathogens are so unique and so feared in the health community that even one case triggers massive response measures (Smallpox, 2007). Treatment for Category B agents is also available through certain common antibiotics, protocols, and methods like IV vasopressors if ricin is ingested (Category Agents, n.d.; Nania, 2013).
Overall, treatment for bioweapon agents is highly available and in the U.S. and some other countries, poses a substantial roadblock for terrorist goals that might include large outbreaks. The U.S. and other industrialized nations (such as Australia and those countries in the European Union) are constantly improving response measures for bioweapons, while health response systems in developing countries are still very rudimentary (Global infectious disease factsheet. 2013). Efforts within the U.S. also focus on improving responses to international health crises and emerging infectious diseases, as borders do not constrict health disasters. Continued efforts to treat and even vaccinate against these pathogens will only make this more of a barrier for potential bioterrorists.
Vaccination capacity in the U.S. is also a considerable hurdle facing some forms of bioterrorism. Smallpox and anthrax both have vaccination programs available that could be mass distributed within several days through the Strategic National Stockpile (SNS). There is also work on vaccine for plague that could be applied (Titball, 2001). Vaccination programs are effective and can be rolled out quickly with Point of Distributions (PODs). PODS are specialized units used to quickly and effectively distribute vaccinations and prophylaxis to large populations. Recent response to pandemic influenza like H1N1 (“swine flu”) made public health systems even more effective in the art of mass vaccination, education, and response measures. After the Amerithrax attacks, President Bush initiated a mass smallpox vaccination program that was later halted, but the effect nonetheless showed that national vaccination production and distribution can occur (Cohen, 2004). Mass vaccination can halt the transmission of disease and prevent the further spreading of infections, as done with polio and smallpox.
Mass Response Measures
Public health preparedness is by no means a new concept, but since the Amerithrax attacks it has attracted more funding and resources. The U.S. public health system has become more attuned to the realistic threats that bioweapons and infectious diseases pose. Federal funding has supplied health departments and related organizations with more personnel training capacity (Koenig, 2007). Public health preparedness and response to bioterrorism and pandemics are common components in public health and healthcare education.
DHS’s Center for Domestic Preparedness offers dozens of fully funded certification courses for first responders and public health personnel. Some may view the recent H1N1 outbreak as an over-hyped pandemic, but the response that took place helped mitigate the spread of the virus (Cressey, 2010). The education that came from H1N1 allowed the public health system to review and change their plans to be more effective and adaptable. Response measures employed in public health emergencies such as pandemics and bioterrorism events involve isolation, quarantine, mass vaccination or prophylaxis (treatment to prevent disease), and education.
Because the presence of public health as a component of preparedness has considerably advanced since the Amerithrax attacks, non-state actors looking to pursue bioterrorism in the U.S. face formidable challenges. The use of PODs, isolation procedures, and mass education will likely reduce the efficacy of such attacks. Earlier attacks like Amerithrax, the Rajneeshees, and small, criminal based attacks such as lab technicians poisoning doughnuts with salmonella, have increased both the awareness and understanding of what a biological attack entails and the tools needed to carry out an attack.
The media attention (television and social media) that the Amerithrax attacks received provided a substantial amount of information to individuals outside the public health system. Current and future response measures are moving away from control methodologies and are now focusing on prevention like syndromic surveillance, creating additional deterrents that can mitigate the impact that bioterrorism events cause (Buehler, 2004; Henning, 2004). The growing ability to quickly identify and respond to outbreaks of disease has the potential to greatly minimize the force of bioweapon attacks.
ATTITUDE OF POTENTIAL USERS
Intentions
The intention of non-state actors considering the use of biological weapons can range across a broad spectrum. Carus points to five motives for terrorists and a sixth motive being considered “criminal” as it primarily involves extortion. The five terrorist motives Carus identified are mass murder (killing specific individuals), murder, incapacitation, political statements, and anti-agriculture (Carus, 2002). Carus found that the primary reasons for terrorists to use bioweapons were to terrorize, cause mass murder, and murder (Carus, 2002). Aum Shinrikyo falls into these categories as they both attempted to kill the Japanese royal family with anthrax, and infect and/or incapacitate large quantities of people via the attempted rooftop dissemination and their sarin attack (Carus, 2002. Rosenau, 2001).
Bruce Hoffman noted that a “terrorist act is conceived and executed in a manner that simultaneously reflects the group’s particular aims and motivations, fits its resources and capabilities, and takes account of the target audience at which the act is directed. The tactics and targets of various terrorist movements, as well as the weapons they favor, are. . .shaped by a group’s ideology, its internal organizational dynamics and the personalities of its key members, as well as a variety of internal and external stimuli” (Tucker, 2000). The internal ideology of a terrorist group must see bioterrorism as an effective form of action, but the group must also have the capabilities and resources to carry out an attack. The attitude of terrorists towards bioterrorism can determine whether they attempt bioweapon development and utilization.
To understand the role of attitude and impact on terrorist action, Tucker noted that there are several characteristics of terrorists groups likely to use chemical or biological weapons:
- Escalatory pattern of violence –groups that show an increase in violence as time progresses, viewing commonly used weapons as archaic and rudimentary.
- Innovation in weapons and tactics, willingness to take risks – the group does not hesitate to deviate from conventional weapons and is willing to work with dangerous weapons.
- Paranoia and grandiosity – the group has an overwhelming paranoia (Aum Shinrikyo was an example, believing that the Japanese government was slowly poisoning them), and views itself as superiors to outsiders.
- Small groups of militants – core groups of radical activists transition to terrorist actions as their organizations and resources grow.
- Isolation, no outside constituency – a closed cult (like Aum Shinrikyo and Rajneeshees) creates a sense of isolation that allows for a psychological removal from society.
- Charismatic leadership – a leader garners extensive support and unwavering dedication and can turn individuals that would normally never attempt crimes into terrorists for organizational goals and acceptance.
- Defensive aggression – a group feels they are waging war against a truly evil adversary and have a survival mentality.
- Apocalyptic ideology – an organization sees itself in battle against an evil in an attempt to reach moral superiority; it also possesses a survivalist mentality.
- Group-think and risk-taking behaviors are also considered to be characteristics of some terrorists groups. (Tucker, 2000).
Cronin has also commented on terrorist attitudes, noting that the use of bioterrorism may be associated with “global availability of CBW information and stockpiles, growth of militant religious groups with political agendas as a percentage of all terrorist groups, internalization of the threat of terrorism, and the clear evidence of terrorist interest and capabilities” (Cronin, 2003). Interestingly, Cronin also points out reasons groups like Al Qaeda might avoid using CBW against the U.S. since “technical difficulties in carrying out such attacks continue to be significant. Aum Shinrikyo is a good example” (Cronin, 2003). Cronin points to several factors related to terrorist mentality that may impact the use of bioweapons: efficacy, complexities not associated with traditional weapons, and the herd mentality in using previously successful tactics (Cronin, 2003). The intention of a terrorist group must support the use of bioweapons for it to move past the initial phases of consideration. For example, a terrorist group that wanted to maximize fear and witnesses while avoiding a societal breakdown might favor bioterrorism. Bioweapons do not impact infrastructure, only people. Biological weapons do not destroy buildings or cause the physical damage that is seen with a bomb or nuclear weapon. Biological weapons also have a temporal expiration in that control measures, whether vaccination, isolation, prophylaxis, or treatment, will eventually stop the spread of disease. Nuclear weapons have long-lasting implications with radiation poisoning, whereas bioweapons do not. The intentions of terrorists groups can either encourage or discourage the use of bioweapons, but this is the initial step to terrorists considering the route. Intentions can be both a barrier and a motivator for bioweapons use.
Media Attention
The function of media and social attention to such attacks may be a considerable hurdle for bioweapons. Some biological weapons, such as foodborne pathogens or plague, can be relatively covert as a result of the time lag associated with their incubation period. While there is a growing trend in unclaimed terrorist activity, the “ambiguity of such attacks may be considered a disadvantage” (Tucker, 2000). The misconception that an outbreak is naturally occurring might very well discredit or disrupt the message such a group is intending to send. In general, outbreaks and health-related news do not gain a lot of media attention, unless it involves a rare organism. There are several natural outbreaks occurring all over the world every day, yet very few people know about them (ProMed, 2013). If media attention and international exposure are a desired outcome, using a biological agent may not meet those needs.
Apocalyptic Ideology
Several studies have pointed to the role of religion and apocalyptic mentality that is found among some terrorist groups. Tucker noted that “some quasi-religious terrorist organization also appear to have a mystical fascination with poisons and disease” (Tucker, 2000). Aum Shinrikyo is a prime example of this. Believing they were defending themselves against the coming apocalypse, Aum leaders stated that they were both preparing themselves for the end, but also attempting to initiate a war between Japan and the U.S. that Aum’s leader, Asahara, had envisioned (Tucker, 2000). Instigating the war would help bring about the apocalypse they had planned for. Cult-like, apocalyptic organizations might have an increased interest in bioweapons, especially if there is a religious component.
View of Bioweapons as WMD’s
The notion that biological weapons are the “poor man’s atomic bomb” has been refuted by studies that have shown that these weapons are neither cheap nor capable of nuclear-level destruction. There is nonetheless a fissure among academics regarding the reality of the bioweapons threat. While some, like Dr. Joshua Lederberg, believe bioweapons to be a major threat, especially with the growing biotechnology field, others like Dr. Milton Leitenberg view the threat to be highly “exaggerated” as a result of the merging of terrorism and biological weapons, which caused bioweapons to receive “undue attention” (Thompson, 2006. Ledgerberg, 1999; Leitenberg, 2006).
Several researchers in the field of bioweapons have pointed to the focus on threat and not on capabilities (ability to acquire, weaponize, and disseminate pathogens), but one must also consider the terrorist view of bioweapons as WMD’s. Considering the lack of damage to infrastructure that bioweapons yield, the outcomes tend to be more death and incapacitation based, and in most cases, are limited in potential numbers of victims. Enemark noted that the “WMD potential of a non-state actor is determined by three factors – the audience, content of message, and degree of social interaction” (Enemark, 2006). These factors may also influence how terrorists view bioweapons as a potential WMD. Religious and cult-like organizations that focus on apocalyptic outcomes might tend to share the ideology that bioweapons fit their needs. In the end, efficacy is in the eye of the beholder, and if non-state actors are unable to balance their goal with the resources, technical hurdles, risks, and necessary expert knowledge involved, they may deem bioweapons unjustifiable.
Conclusions
SUMMARY OF BARRIERS
This summary is qualitative and is based on the case studies reviewed and general findings from the literature. The greatest barriers are dissemination and weaponizing of a bioweapon agent. Technical components, dissemination, and weaponization involve extensive professional expertise, equipment, and resources. The attitude of potential users is probably a somewhat less robust hurdle, since it will vary with whether a group is willing to deviate from traditional practices, and if its intentions are aligned with the expected outcome of bioterrorism.
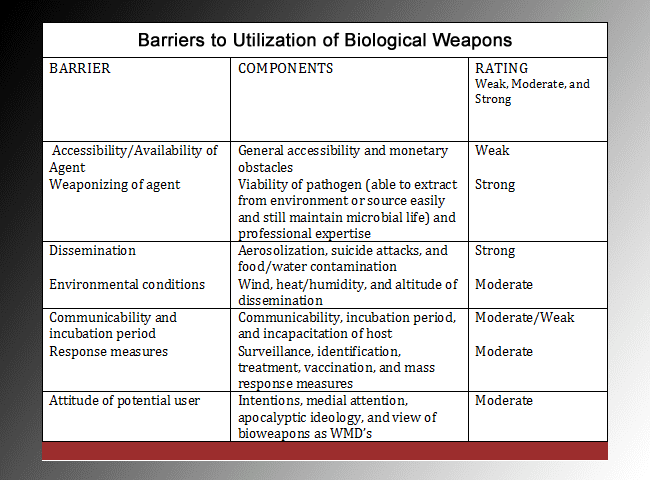
Response measures and environmental issues do pose considerable hurdles to potential users, but non-state actors can use specific dissemination methods or pathogens to reduce these barriers. The least significant hurdles to bioweapon use are accessibility of the agents and consideration for communicability. Rajneeshees and Aum both established that pathogens used as bioweapons are easy to purchase. While availability may have changed in recent years, the dual-use dilemma makes equipment and cultures relatively easy to obtain. Communicability has a unique role as a barrier in that it poses a dual rating as a moderate barrier from a technical standpoint, but does not seem to be much of hurdle in regards to the intent of potential users. The moderate rating for communicability relates to the limitations of certain bioweapons that produce no secondary cases in their actual impact. Given some groups’ past fascination with anthrax and botulism, neither of which is communicable, it is conceivable that terrorist organizations may not consider communicability when evaluating bioterrorism as an effective tactic.
AREAS FOR MORE RESEARCH
The reality of bioweapons threat assessments has becoming increasingly debated. While there are some like Carus and Koblentz that view the threat as very real and imminent, others like Vogel and Leitenberg pose questions about the realistic capabilities of terrorists and if bioweapons truly fit their organizational goals. Several academics emphasize the technical barriers that prevent bioterrorism from being used as successfully as bombs and other traditional tactics.
Technological innovations can both hinder and facilitate bioweapons use. Bioterrorism is especially affected by technical advances, as the biggest hurdles lie in most groups’ lack of technical and expert knowledge. Mintz has noted that the availability of equipment and the knowledge to use it has become more accessible, allowing less-skilled individuals to easily access ready-to-make kits. Mintz also points to the advancements in biological engineering that allows scientists to genetically alter and engineer pathogens for specific uses (Mintz, 2005). Tucker has pointed to the concern over growing availability of CBW and increasingly aggressive organizations (Tucker, 2000). Microbiology is making leaps and bounds every year, however, there are still concerns over zoonotic diseases, spillover (uncommon diseases jumping species as a result of environmental infringements), and the genetic mutation of several viruses.
Drug-resistant organisms have also become a concern, as they pose serious threats to treatment and public health. Rare cases of multi-drug resistant tuberculosis require quarantine and severe medical intervention. The potential for terrorists to make pathogens drug-resistant is one of huge concern. Many bioweapons experts, like Vogel, point to the biotechnology revolution that provides things like black box technology, fuzzy logic in medical applications, and publishing the full genome of Category A agents (in 2012, a group of British scientists published the full genome of Y. pestis in the Nature journal) as a potential source for increased bioterrorism application (Vogel, 2013).
Based on this assessment, there are several areas where additional research is needed. Identifying breaks in the chain to pathogen access is necessary to reduce the ease of availability. Emphasis on public health education regarding both pathogen accessibility and intentional versus naturally occurring outbreaks would better prepare the public health system to prevent and respond to bioterrorism events.
Lastly, it is crucial to shift the focus of preparedness and threat assessment from solely vulnerability to also address the capabilities and intent of potential users. Better understanding of these components will allow future policy and public health system changes to protect vulnerable points, but also to reinforce existing hurdles to bioterrorism. Strengthening the roadblocks potential non-state users may encounter will help prevent future use of bioweapons. In all, the gap between popular assumptions about bioterrorism and its actual use is a result of the considerable hurdles and barriers non-state actors must overcome to employ bioweapons.
REFERENCES
Ackerman G., Moran K. (2006). Bioterrorism and Threat Assessment. The Weapons of Mass Destruction Commission, 22. Retrieved from: http://www.un.org/disarmament/education/wmdcommission/files/No22.pdf.
Alchon, Suzanne Austin. A Pest in the Land: New World Epidemics in a Global Perspective. (2003). University of New Mexico Press, New Mexico.
Arizona Department of Health Services (ADHS). (n.d.). Bureau of Epidemiology and Disease Control: Office of Infectious Disease Services: Arizona Administrative Code. Retrieved November 10, 2013, from http://www.azdhs.gov/phs/oids/code.htm.
Bain B., Masbath, M., Cirincione, J. (March 16, 2006). Exaggerating the Threat of Bioterrorism. Proliferation Analysis, Carnegie Endowment for International Peace.
Banks, H. T., & Chávez, C. (2003). Bioterrorism: mathematical modeling applications in homeland security. Philadelphia, PA: Society for Industrial and Applied Mathematics.
Buehler J., Hopkins R., Overhage J., Sosin D., Tong V. (2004). Framework for Evaluating Public Health Surveillance Systems For Early Detection of Outbreaks: Recommendations from the CDC working group. MMWR (CDC), 53(RR-5):1-13.
Carus, W. (2002). Bioterrorism and Biocrimes: The Illicit Use of Biological Agents Since 1900. Amsterdam, Netherlands: Fredonia Books.
Carus, W. (1991). “The Poor Man’s Atomic Bomb?” Biological Weapons in the Middle East. The Washington Institute for Near East Policy, Policy Papers, 23.
“CDC Smallpox | Smallpox Overview.” Centers for Disease Control and Prevention Emergency Preparedness & Response Site. N.p., n.d. Web. 14 Sept. 2013. http://www.bt.cdc.gov/agent/smallpox/overview/disease-facts.asp.
“CDP: Center for Domestic Preparedness”. (n.d.). Department of Homeland Security. Accessed on October 22, 2013 from: https://cdp.dhs.gov.
Category Agents. (n.d.). CDC | Bioterrorism Agents/Diseases (by Category) | Emergency Preparedness & Response. CDC Emergency Preparedness & Response Site. Retrieved September 10, 2013, from http://www.bt.cdc.gov/agent/agentlist-category.asp#c.
Chapter 2: Assessing Risk: Threats, Vulnerabilities and Capacities. (n.d.). Front Line. Retrieved May 6, 2013, from http://www.frontlinedefenders.org/book/export/html/542.
Cirincione, J., Wolfsthal, J. B., & Rajkumar, M. (2002). Deadly Arsenals: Tracking Weapons of Mass Destruction. Washington, D.C.: Carnegie Endowment for International Peace.
Cohen, H., Gould, R., Sidel ,V. (2004). The Pitfalls of Bioterrorism Preparedness: the Anthrax and Smallpox Experiences. Am J Public Health, 94(10):1667-1671.
Cosgrove, S,. Perl, T., Song, X., Sisson, S. (2005). Ability of Physicians to Diagnose and Manage Illness Due to Category A Bioterrorism Agents. Arch Intern Med; 265:2002-2006.
Crane, J., McCluskey, J., Johnson, G., Harbison, R. (2010). Assessment of community Healthcare Providers Ability and Willingness to Respond to Emergencies Resulting From Bioterrorist Attacks. J Emerg Trauma Shock; 3(1): 13-20.
Cressey, D. (2010, January 27). Nature News Blog. Retrieved October 22, 2013, from http://blogs.nature.com/news/2010/01/who_fights_claims_h1n1_pandemi.html
Cronin, Audrey. (2003). Terrorist Motivations for Chemical and Biological Weapons Use: Placing the Threat in Context. Report for Congress, RL31831, March 28, 2003.
Dando, M. (2006). Bioterror and Biowarfare: A Beginner’s Guide. Oxford, England: Oneworld Publications
Enemark, C. (2006). Biological Attacks and the Non-state Actor: A Threat Assessment. Intelligence and National Security, 21 (6).
Evans, Robert. (July, 2013). Personal interview regarding ricin use in Maricopa County, Arizona.
Falkenrath, R. A., Newman, R. D., & Thayer, B. A. (1998). America’s Achilles’ heel nuclear, biological, and chemical terrorism and covert attack. Cambridge, Mass.: MIT Press.
Federal Bureau of Investigation — Amerithrax Investigation. (n.d.). FBI — Homepage. Retrieved September 7, 2013, from http://www.fbi.gov/about-us/history/famous-cases/anthrax-amerithrax/amerithrax-investigation.
Fidler, D. P., & Gostin, L. O. (2008). Biosecurity in the Global Age: Biological Weapons, Public Health, and the Rule of Law. Stanford, Calif.: Stanford Law and Politics.
Fletcher, Holly. (2012). Aum Shinrikyo. Council on Foreign Relations. Retrieved on September 8 2013 from http://www.cfr.org/japan/aum-shinrikyo/p9238#p3.
Fox, J. (2002). Bioterrorism Threat Brings Changes to Microbiology on Several Fronts. ASM News, 68 (10).
Garza, A. (June, 2013). Ricin: the Very Poor Man’s Toxic Terror. The Pandora Report. George Mason University Biodefense Graduate Program.
Gerstein, D. (2009). Bioterror in the 21st Century. Annapolis, MD: Navy Institute Press.
Global Infectious Disease Surveillance. (2013). WHO. Retrieved November 4, 2013, from http://www.who.int/mediacentre/factsheets/fs200/en/
Guillemin, J. (2005). Biological Weapons: From the Invention of State-Sponsored Programs to Contemporary Bioterrorism. New York City, NY: Columbia Press.
Hansen, L. (1990). Biological and Toxin Weapons: Arms Control, Stability, and Western Security. Politics and the Life Sciences, 9(1): 47-58
Harris, R., & Paxman, J. (2002). A Higher Form of Killing: The Secret History of Chemical and Biological Weapons. London, UK: Random House Press
Hellmich C., Redig, A. (2007). The Question is When: The Ideology of Al Qaeda and the Reality of Bioterrorism. Studies in Conflict & Terrorism, 30:375-396.
Henning, Kelly J. (September 24, 2004). Overview of Syndromic Surveillance: What is Syndromic Surveillance? CDC MMWR, 53(Suppl);5-11.
Heymann, D. L. (2008). Control of Communicable Diseases Manual (19th ed.). Washington, DC: American Public Health Association.
Hinson, T. (2013, April 8). Could Smallpox Really Be Turned Into a Biological Weapon by Terrorists? | Metro News. Metro.co.uk: News, Sport, Showbiz, Celebrities from Metro Newspaper. Retrieved July 10, 2013, from http://metro.co.uk/2013/04/08/could-smallpox-really-be-turned-into-a-biological-weapon-by-terrorists-3585028/.
Hurt-Mullen K., Coberly J. (2005). Syndromic Surveillance on the Epidemiologist’s Desktop: Making Sense of Much Data. MMWR (CDC),54(Suppl), 141-147.
Johnson, L. (n.d.). Is Al Qaeda Making Anthrax? – CBS News. Breaking News Headlines: Business, Entertainment & World News – CBS News. Retrieved August 31, 2013, from http://www.cbsnews.com/8301-18563_162-577395.html.
Johnson, T. J. (n.d.). A History of Biological Warfare from 300 BCE to the Present. AARC. Retrieved June 4, 2013, from https://www.aarc.org/resources/biological.
Kaplan, E., Craft, D., Wein, L.(2002). Emergency Response to a Smallpox Attack: the Case for Mass Vaccination. Proceedings of the National Academy of Sciences of the United States of America: 99(6):10935-10940.
Koblentz, G. (2009). Living Weapons: Biological Warfare and International Security. Ithaca, NY: Cornell University Press.
Koenig, R. (2011, October 7). Join The Beacon. St. Louis Beacon. Retrieved October 22, 2013, from https://www.stlbeacon.org/#!/content/1505
Krämer, Alexander, Mirjam Kretzschmar, and Klaus Krickeberg. Modern Infectious Disease Epidemiology Concepts, Methods, Mathematical Models, and Public Health. New York: Springer, 2010. Print.
Leard, Jason. (Director) (2013, October 18). Bioterrorism and Public Health. SAFER. Lecture conducted from SAFER, Tucson, AZ.
Lederberg, Joshua. (1999). Biological Weapons: Limiting the Threat. BCSIA Studies in International Security. Cambridge, MA: MIT Press.
Leitenberg, Milton. (December 2005). Assessing the Biological Weapons and Bioterrorism Threat. Carlisle, PA: Strategic Studies Institute, U.S. Army War College, Title 17, Section 101.
Leitenberg, Milton. (February 17, 2006). Bioterrorism Hyped. Los Angeles Times. Retrieved on November 10, 2013 from: http://articles.latimes.com/2006/feb/17/opinion/oe-leitenberg17.
Lewis, R. (n.d.). No Mass Smallpox Vaccination in US | The Scientist Magazine®. The Scientist Magazine®. Retrieved September 1, 2013, from http://www.the-scientist.com/?articles.view/articleNo/21334/title/No-mass-smallpox-vaccination-in-US/.
Lowen, Anice C., Samira Mubareka, John Steel, and Peter Palese. “Influenza Virus Transmission Is Dependent On Relative Humidity And Temperature.” PLoS Pathogens 3.10 (2007): e151. Print.
Lyell, L. (1996). Chemical and Biological Weapons: The Poor Man’s Bomb. North Atlantic Assembly Committee. October 4, 1996.
Malet, D., Rogers H. (Summer/Fall 2010). Biological Weapons and Security Dilemmas. The Whitehad Journal of Diplomacy and International Relations.
Mayor, A. (2003). Greek Fire, Poison Arrows, and Scorpion Bombs: Biological and Chemical Warfare in the Ancient World. Woodstock: Overlook Duckworth.
Mintz, J. (n.d.). Technical Hurdles Separate Terrorists From Biowarfare (washingtonpost.com). The Washington Post: National, World & D.C. Area News and Headlines – The Washington Post. Retrieved September 1, 2013, from http://www.washingtonpost.com/wp-dyn/articles/A35011-2004Dec29.html
Moye, P., Pesik, N., Terndrup,T., Roe, J., Weissman, N., Kiefe, C., Houston, T. (2007). Bioterrorism Training in U.S. Emergency Medicine Residencies: Has It Changed Since 9/11? Acad Emerg Med. Mar;14(3): 221-227.
Nania, J. MD. (2013, September 2). Personal Interview
NNDSS | National Notifiable Diseases Surveillance Systems.” http://www2.cdc.gov/Default.htm. N.p., n.d. Web. 22 Oct. 2013. http://wwwn.cdc.gov/nndss/.
Nordmann, B. (November 1, 2010). Issues in Biosecurity and Biosafety. International Journal of Antimicrobial Agents. Retrieved on October 28, 2013 from: http://www.state.gov/t/avc/rls/164668.htm.
Oldston, Michael. Viruses, Plagues, & History. 2010. Oxford University Press. New York City, New York.
Preston, Richard. The Demon in the Freezer: A True Story. 2003. Fawcett, New York City, New York.
ProMed. (2013). International Society for Infectious Diseases. Retrieved on October 21, 2013 from: http://www.promedmail.org.
Purver, R. G. (1995). Chemical and Biological Terrorism: The Threat According to the Open Literature. Ottawa, Ontario: Canadian Security Intelligence Service.
Radosavljevic, V., Belojevic, G., Jovanovic, L. (2012). A Mathematical Model of Bioterrorist Attack Risk Assessment. Bioterrorism & Biodefense, 3(1).
Ray, E., & Schaap, W. H. (n.d.). Bioterror Manufacturing Wars The American Way Edited by Ellen Ray and Willam H. Schaap. Third World Traveler, third world, United States foreign policy, alternative media, travel. Retrieved July 9, 2013, from http://www.thirdworldtraveler.com/Weapons/Bioterror.html.
Reppert, B. (n.d.). AIBS Washington Watch | The Biodefense Buildup: Fallout for Other Research Areas?. American Institute of Biological Sciences. Retrieved September 19, 2013, from http://www.aibs.org/washington-watch/washington_watch_2005_04.html
Rogers, E. M. (1983). Diffusion of Innovations (3rd ed.). New York: Free Press.
Rosenau, Wiliam. (2010). Aum Shinrikyo’s Biological Weapons Program: Why Did It Fail? Studies in Conflict & Terrorism, 24:4, 289-301.
Rosenberg, B. H. (n.d.). Anthrax Attacks Pushed Open an Ominous Door . Home | Jonathan and Karin Fielding School of Public Health. Retrieved September 1, 2013, from http://articles.latimes.com/2002/sep/22/opinion/op-rosenberg22.
Schmid, A. (1999). Terrorism and the Use of Weapons of Mass Destruction: From Where the Risk? Terrorism and Political Violence, 11:4, 106-132.
Simon, J. D. (1994). The Terrorist Trap: America’s Experience with Terrorism. Bloomington: Indiana University Press.
Spiers, E. (2010). A History of Chemical and Biological Weapons. London, UK: Reakion Books.
Shane, S. (n.d.). Everyone Has an Anthrax Theory. Jonathan and Karin Fielding School of Public Health. Retrieved September 2, 2013, from http://www.ph.ucla.edu/epi/bioter/everyoneanthraxtheory.html.
Shane, S. (2010, February 19). F.B.I. Concludes Investigation in Fatal Anthrax Mailings – NYTimes.com. The New York Times – Breaking News, World News & Multimedia. Retrieved September 13, 2013, from http://www.nytimes.com/2010/02/20/us/20anthrax.html?pagewanted=2&_r=0&ref=bruceeivins.
Smallpox Response Plan and Guidelines (Version 3.0). (2007, February 6). CDC Smallpox. Retrieved October 22, 2013, from http://www.bt.cdc.gov/agent/smallpox/response-plan/.
“Stages.” Academic Computer Center. N.p., n.d. Web. 15 Sept. 2013. http://academic.pgcc.edu/~kroberts/Lecture/Chapter%2014/stages.html.
Stern, Jessica. (2000). Terrorist Motivations and Unconventional Weapons. Harvard John F. Kennedy School of Political Science.
“Surveillance for Infectious Disease.” Boston University School of Public Health | Home Page. N.p., n.d. Web. 17 Sept. 2013. Retrieved on September 13 from: http://sph.bu.edu/otlt/MPH-Modules/EP/EP713_Surveillance/EP713_Surveillance4.html.
Syndromic Surveillance: Reports from a National Conference. (2004). Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report (Suppl):53, 1-264. APC. Update to Syndromic Surveillance Implementation Guide. May 2008. Accessed on October 31, 2013 from: http://www.cdc.gov/mmwr/preview/su5301toc.htm.
Titball, R. (2001). Vaccination Against Bubonic And Pneumonic Plague. Vaccine, 19(30), 4175-4184.
Thompson, C. (2006). The Bioterrorism Threat By Non-state Actors: Hype or Horror? Monterey Naval Postgraduate School.
Tucker, J. B. (2000). Toxic terror: Assessing Terrorist Use of Chemical and Biological Weapons. Cambridge, Mass.: MIT Press.
United Nations Office for Disarmament Affairs – The Biological Weapons Convention. (n.d.). Welcome to the United Nations: It’s Your World. Retrieved September 12, 2013, from http://www.un.org/disarmament/WMD/Bio/.
Vogel, K. (2013). Phantom Menace or Looming Danger? A New Framework for Assessing Bioweapons Threats. Baltimore, MD: John’s Hopkins Press.
Wheelis, M., Dando M. (2003). Back to Bioweapons? Bulletin of the Atomic Scientists, 59 (1): 40.
Zanders, Jean Paul. (1999). Assessing the Risk of Chemical and Biological Weapons Proliferation to Terrorists. The Nonproliferation Review, 6(4): 30.
Zubay, G. L. (2005). Agents of Bioterrorism: Pathogens and Their Weaponization. New York: Columbia University Press.